
Understanding Diuretic Resistance
A guide from Resistance to Precision: A Phenotype-Based Approach for acute care physicians

From:-
Dr Arihant Jain, MD | lifeonthefrontline.com
Instagram: @humans.of.em
X - dr__hunt
PART 1 — Understanding Diuretic Resistance
The problem
Loop diuretics are the cornerstone of decongestion—yet:
20–30% of patients fail to respond adequately
Associated with longer hospital stay, ICU need, and mortality
What is Diuretic Resistance?
Failure to achieve negative sodium and fluid balance despite adequate dosing
Often misdiagnosed
Many cases are actually a result of:
Under-dosing
Poor drug delivery
Wrong physiology
PART 2 — Mechanisms of Diuretic Resistance
(This is the key to everything that follows)
Diuretic resistance is multifactorial, driven by 3 major pathways:
1️⃣ Pharmacokinetic Failure (Drug never reaches kidney)
Gut edema → ↓ oral absorption
Low cardiac output → ↓ renal perfusion
High CVP → renal congestion
Hypoalbuminemia → altered drug delivery
👉 Result: insufficient drug at site of action
2️⃣ Tubular Adaptation (“Nephron fights back”)
Chronic loop use → distal nephron hypertrophy
↑ Na-Cl cotransporter (NCC)
↑ ENaC activity
👉 Result: distal sodium reabsorption overrides loop effect
3️⃣ Neurohormonal Activation (“Body wants sodium”)
RAAS activation
Sympathetic activation
Vasopressin
👉 Creates a state of “basal sodium avidity”
👉 Kidney is primed to retain sodium despite diuretics
The Forgotten Player — Chloride
Hypochloremia → activates WNK kinases
↑ Sodium reabsorption
↓ Diuretic response
👉 Diuretics worsen chloride depletion → vicious cycle
Diuretic resistance is NOT just “need more dose”
It’s a mismatch between drug, kidney, and physiology
Read further about pathophysiology behind Diuretic Resistance here
PART 3 — How to Monitor Diuretic Therapy in ED
(Where most clinicians go wrong)
❌ What NOT to rely on:
Weight
Fluid balance charts
“Urine looks good”
👉 These do NOT reflect sodium removal
✅ What actually matters:
1. Urinary Sodium (U. Na+) — THE GOLD STANDARD
⏱ Check 1–2 hours after IV diuretic
>70 mmol/L → Adequate response
<50–70 mmol/L → Resistance
👉 This predicts response before clinical deterioration
2. Urine Output
Target: >100–150 mL/hour (first 6 hours)
3. Bedside Ultrasound
Lung B-lines → pulmonary congestion
VExUS → systemic venous congestion
Dynamic Monitoring with all 3 adjuncts.
Assess → Adjust → Reassess every 2–6 hours
Not next morning. Not after ward transfer.
PART 4 — The Shift: Phenotype-Based Diuretic Therapy
Same drug. Same dose. Different patients → different failures.
👉 That’s because different mechanisms dominate in different phenotypes
PHENOTYPE 1 — RIGHT HEART FAILURE
“Venous congestion is the problem”
🔬 Mechanism
↑ CVP → renal congestion
↓ renal perfusion gradient
↓ drug delivery
Strategy
Aggressive decongestion (even if borderline BP)
Higher loop doses
Early combination therapy
If low output:
Add inotropes (dobutamine/milrinone)
Use norepinephrine if hypotensive
👉 Decongestion improves renal function
PHENOTYPE 2 — ADVANCED CKD
“Delivery + tubular resistance”
Mechanism
↓ tubular secretion
Chronic sodium retention
Distal nephron adaptation
Strategy
Use higher loop doses (expected)
Prefer IV route
Early add-ons:
Acetazolamide → if metabolic alkalosis
Thiazide → if chronic loop use
👉 Sequential nephron blockade is essential
Critical points:
Correct chloride
Accept mild creatinine rise
PHENOTYPE 3 — OBESITY
“Hidden congestion + neurohormonal activation”
Mechanism
Adipose tissue → RAAS + SNS activation
↑ plasma volume
↑ intra-abdominal pressure → ↓ renal perfusion
Strategy
Assume underestimated congestion
Use higher doses early
Early combination therapy
Add:
SGLT2 inhibitors (if appropriate)
Clinical pearl
BNP & exam are unreliable → rely on physiology
PHENOTYPE 4 — ELDERLY / FRAIL
“Balance between diuresis and harm”
Mechanism
Altered pharmacokinetics
↓ renal reserve
High vulnerability
Strategy
Gradual decongestion
Close monitoring
Use:
Urine output
UNa
Ultrasound
Goal:
👉 Not aggressive fluid removal
👉 Stable euvolemia + preserved function
Putting It All Together (ED Algorithm)
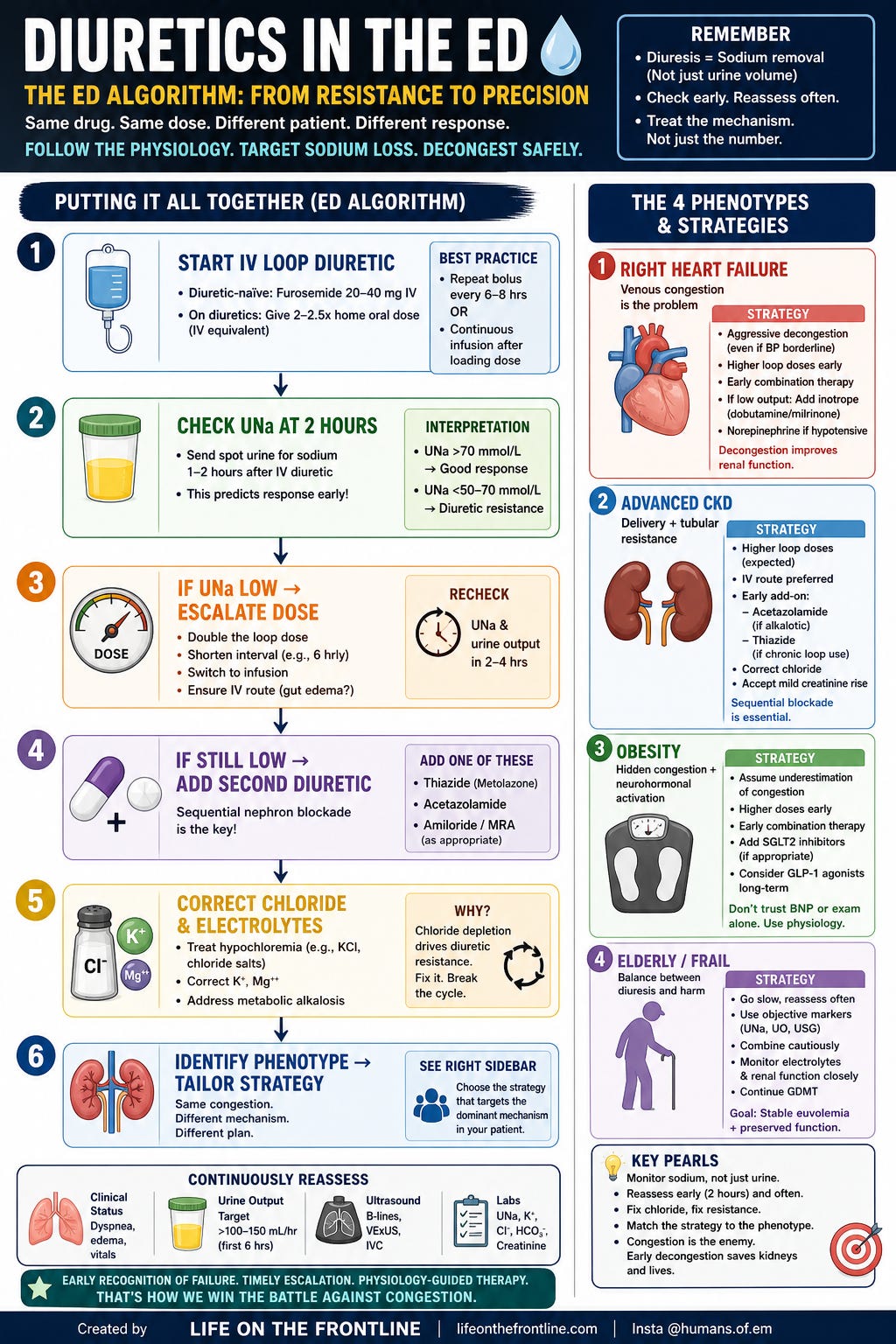
Based on :-
Aletras G, Bachlitzanaki M, Stratinaki M, Foukarakis E, Petrakis I, Pantazis Y, Hamilos M and Stylianou K (2026) Diuretic resistance in cardiorenal syndrome: mechanisms, monitoring and phenotype-tailored management. Front. Cardiovasc. Med. 12:1731305. doi: 10.3389/fcvm.2025.1731305
FINAL TAKEAWAY
Diuretic resistance is not about the drug.
It is about which physiological barrier is dominant.
When you:
Monitor early
Identify mechanism
Treat phenotype
👉 Diuretics start working again.