
Troponin Is Not an MI Test: Part - 2
A New Mental Model for Acute Care Physicians

By-
Dr Arihant Jain, MD | lifeonthefrontline.com
Instagram: @humans.of.em
X | Linkedin | ORCID

Let’s start from where we left in Part -1.
Step Three:
Is There Evidence of Ischemia?
An elevated troponin is a laboratory finding. Ischemia is a clinical diagnosis. And this distinction changes everything.
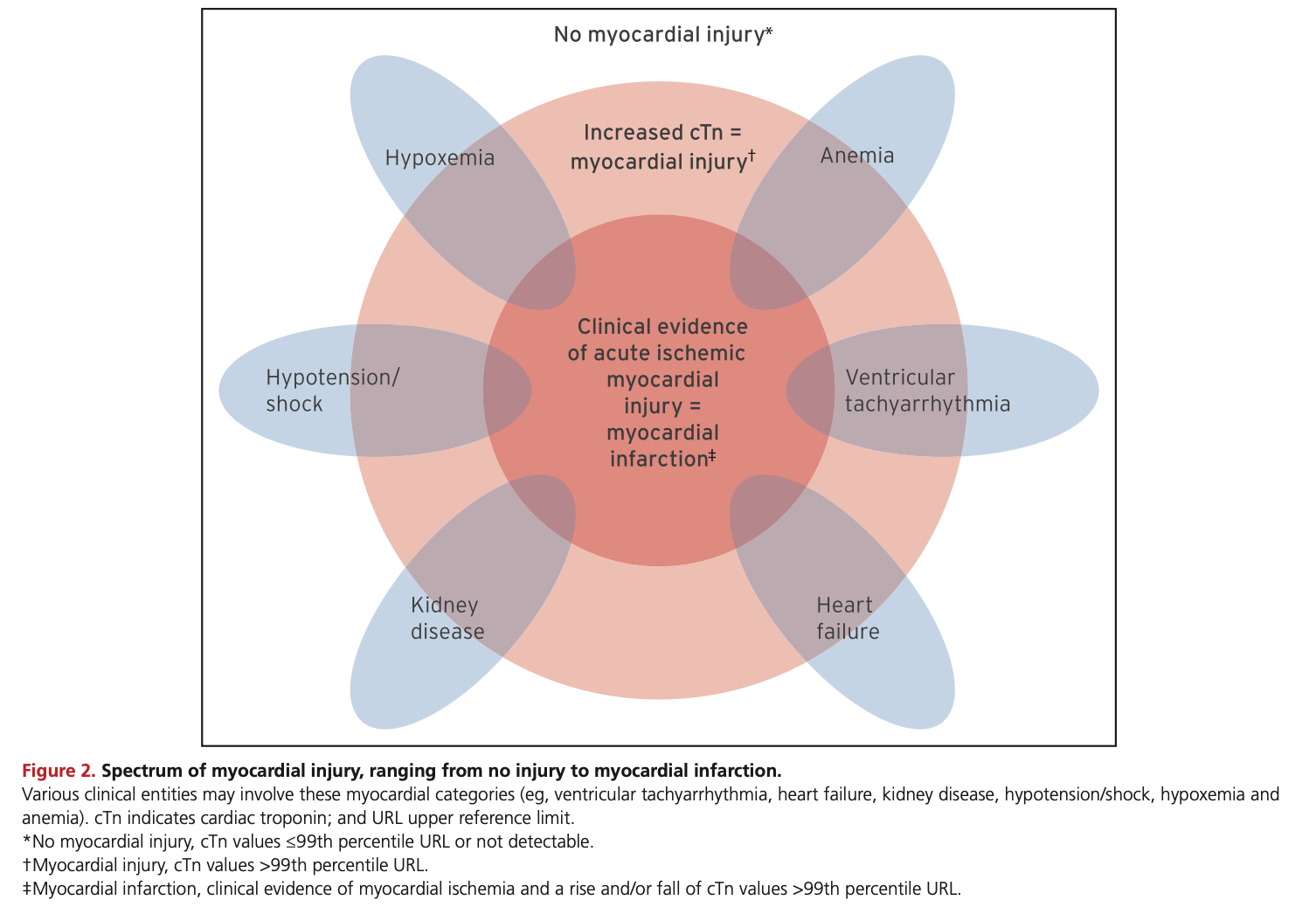
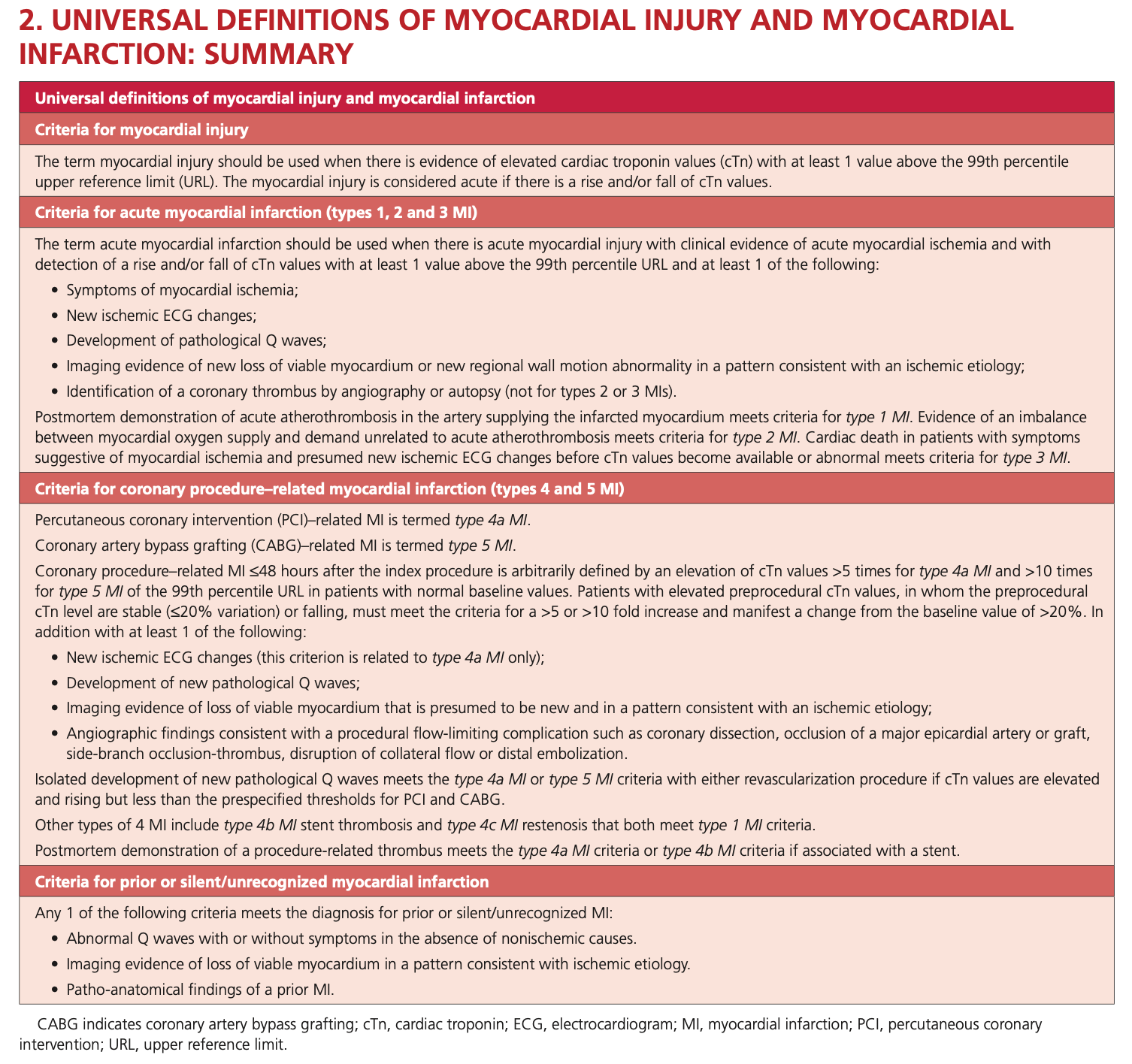
The Fourth Universal Definition of Myocardial Infarction requires
Acute myocardial injury plus evidence of acute myocardial ischemia to establish the diagnosis of myocardial infarction (Thygesen et al., 2018).
That evidence for myocardial ischemia may include:
Symptoms suggestive of myocardial ischemia.
New ischemic ECG changes.
Development of pathological Q waves.
Imaging evidence of new regional wall motion abnormalities.
Identification of a coronary thrombus by angiography or autopsy (Thygesen et al., 2018).
Without ischemia, there is no myocardial infarction. There is only myocardial injury.
The Forgotten Truth
For years, clinicians learned a dangerous shortcut:
Elevated troponin = NSTEMI.
High-sensitivity assays have exposed the flaws in that thinking.
As Rokos, Mattu, and Jaffe emphasize, a substantial proportion of elevated troponin values encountered in contemporary practice arise from conditions entirely unrelated to acute coronary syndromes (Rokos, Mattu, & Jaffe, 2025).
The biomarker is extraordinarily sensitive. It is not extraordinarily specific. The physician must provide the specificity.
The Troponin Matrix
A more useful framework is to think in four quadrants:
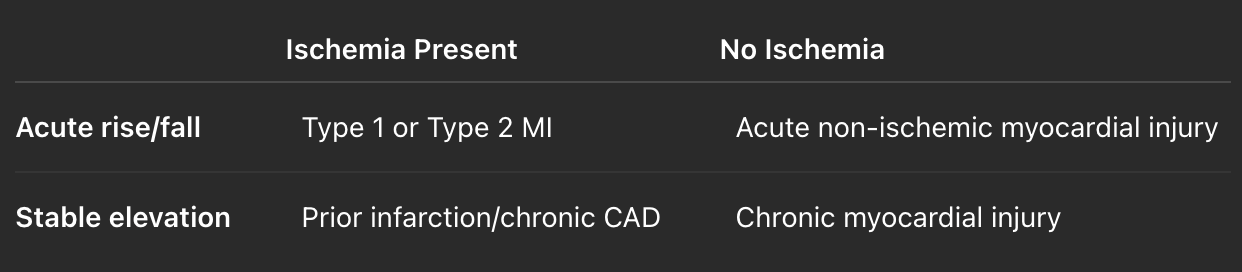
This simple matrix explains why two patients with identical troponin values may require entirely different management strategies. The number alone never tells the whole story.
Type 1 Myocardial Infarction:
The Classical Paradigm
Type 1 MI remains the condition most clinicians immediately think of when they encounter elevated troponin levels.
It results from:
Plaque rupture.
Plaque erosion.
Coronary thrombosis.
Acute atherothrombotic occlusion (Thygesen et al., 2018).
The pathophysiology is straightforward: A disrupted plaque causes coronary obstruction, leading to myocardial ischemia, necrosis, and biomarker release.
This is the disease for which our traditional ACS therapies were designed:
Dual antiplatelet therapy.
Anticoagulation.
Early angiography.
Revascularization.
The challenge is that not every elevated troponin belongs in this category.
Type 2 MI:
The Most Misunderstood Diagnosis in Acute Care
Perhaps no concept creates more confusion than Type 2 myocardial infarction.
The Fourth UDMI defines Type 2 MI as:
Acute myocardial injury with evidence of ischemia resulting from an imbalance between myocardial oxygen supply and demand, unrelated to acute coronary thrombosis (Thygesen et al., 2018).
Examples include:
Severe anemia.
Sustained tachy-arrhythmias.
Hypertensive emergencies.
Profound hypotension.
Coronary vasospasm.
Severe hypoxemia.
Importantly:
Type 2 MI still requires ischemia. That sentence deserves repetition.
Type 2 MI still requires ischemia.
A septic patient with elevated troponin but no ischemic symptoms, ECG changes, or imaging evidence does not automatically have Type 2 MI.
They may simply have acute non-ischemic myocardial injury. This distinction matters because inappropriate labeling influences:
Cardiology referrals.
Antiplatelet prescriptions.
Long-term diagnoses.
Insurance coding.
Patient expectations.
Sometimes, the most accurate diagnosis is also the simplest:
Acute myocardial injury secondary to sepsis.
No infarction. No thrombosis. No unnecessary complexity.
The Trop-Zone Concept:
Thinking Beyond Positive and Negative
One of the most elegant recent approaches to high-sensitivity troponin interpretation comes from Rokos, Mattu, and Jaffe (2025). Rather than forcing clinicians through increasingly complex algorithms, they propose thinking in terms of Troponin Zones.
This framework aligns naturally with bedside decision-making.
Zone 1:
The Whisper Zone
Very low values. Typically near the limit of quantification. The myocardium is quiet. For many assays, extremely low troponin levels carry an exceptionally high negative predictive value for acute MI (Rokos, Mattu, & Jaffe, 2025).
But caution remains essential:
Early presenters may still evolve. Clinical context always supersedes a single number.
Zone 2:
The Thinking Zone
Values around the 99th percentile. This is where emergency medicine earns its salary.
The diagnosis depends upon:
Serial measurements.
Delta changes.
Symptoms.
ECG findings.
Risk factors.
Alternative explanations.
Here, the question shifts from:
“Is the troponin elevated?”
to:
“Why is it elevated?”
Zone 3:
The Alarm Zone
Substantially elevated values. The probability of infarction rises. But certainty remains elusive. Massive troponin elevations may occur in:
Fulminant myocarditis.
Takotsubo syndrome.
Massive pulmonary embolism.
Septic shock.
Electrical storms.
Type 1 MI.
Magnitude informs probability. It does not establish diagnosis. The heart only has a limited vocabulary. Troponin is one of its distress signals. It does not tell us why it is suffering.
The Delta:
The Most Important Number You Never Memorized
High-sensitivity assays changed our relationship with time. The absolute troponin value matters. The trend often matters more.
As Januzzi and colleagues noted, one of the greatest advantages of high-sensitivity assays is their ability to detect very small changes over short intervals (Januzzi et al., 2019).
The second troponin frequently provides information that the first cannot. Think of it this way:
The first troponin is a photograph.
The delta is a movie.
Movies tell better stories. A stable troponin suggests chronic injury. A dynamic change suggests an acute process. What remains is determining whether that process is ischemic.
The Five Questions Every Troponin Demands
This is perhaps the most useful bedside framework.
Question 1:
Is the troponin above the 99th percentile?
If no:
No myocardial injury currently.
Do follow up troponin still if high clinical suspicion.
If yes:
Proceed.
Question 2:
Is there a rise or fall?
If yes:
Acute myocardial injury.
If no:
Chronic myocardial injury.
Question 3:
Is there evidence of ischemia?
Look for:
Symptoms.
ECG changes.
Imaging findings.
Angiographic evidence.
No ischemia?
Stop calling it MI.
If clinical evidence of Ischemia is present.
Repeat Trop, if initially below 99th centile,
monitor patients, repeat ECGs, keep cardiologist in loop.
Question 4:
If ischemia exists, why?
Type 1 to 5 MI.
Question 5:
What disease process explains the injury, if no evidence of myocardial ischemia?
Sepsis?
Pulmonary embolism?
Heart failure?
Myocarditis?
Arrhythmia?
Renal disease?
The troponin tells us that myocardium has suffered. It is our responsibility to determine why.
Three Patients, Three Diagnoses
Case One:
The Septic Patient
A 72-year-old woman with septic shock. Troponin rises from 24 ng/L to 68 ng/L. No chest pain. No ischemic ECG changes. Bedside echo shows global hyperdynamic function.
Diagnosis?
Acute non-ischemic myocardial injury secondary to sepsis.
Not NSTEMI. Not Type 2 MI. The injury is real. The ischemia is absent.
Case Two:
The Tachyarrhythmia Patient
A 58-year-old man presents with atrial fibrillation at 180 beats per minute. Chest discomfort occurs during the episode. Troponin rises from 18 ng/L to 95 ng/L. Diffuse ST depressions resolve after rate control.
Diagnosis?
Type 2 myocardial infarction due to oxygen supply-demand mismatch.
Acute injury. Evidence of ischemia. No plaque rupture.
Case Three:
The Dialysis Patient
A chronic hemodialysis patient presents with pneumonia.
Troponin is 140 ng/L.
Repeat value six hours later remains 142 ng/L. NO symptoms suggestive of ACS. No ischemic ECG changes.
Diagnosis? Chronic myocardial injury.
The elevated number is background information. The stability is the key.
The New Philosophy of Troponin
The era of:
Positive versus negative
is over.
The era of:
Injury versus infarction
has begun.
High-sensitivity assays did not simply improve diagnostics. They forced us to rethink the biology of myocardial damage itself.
They taught us that:
Injury can be acute or chronic.
Acute injury can be ischemic or non-ischemic.
Infarction is only one subset of myocardial injury.
The biomarker became more precise. Our thinking must become equally precise.
Final Reflections
The next time someone tells you:
“The troponin is positive i.e. above 99th percentile URL.”
Pause.
Ask five questions.
Is there injury? Is it acute? Is it ischemic? If ischemic, is it Type 1 or Type 2?
And what underlying disease process explains it? Because the elevated troponin is rarely the diagnosis. It is the heart asking for context. And modern acute care begins by listening carefully to that question.
References
Januzzi JL Jr, Mahler SA, Christenson RH, et al. Recommendations for institutions transitioning to high-sensitivity troponin testing. Journal of the American College of Cardiology. 2019;73(9):1059-1077.
Rokos IC, Mattu A, Jaffe AS. High-sensitivity troponin zones: An alternative approach to clinical decisions. The Journal of Emergency Medicine. 2025.
Thygesen K, Alpert JS, Jaffe AS, et al. Fourth universal definition of myocardial infarction (2018). Circulation. 2018;138:e618-e651.