
Troponin Is Not an MI Test: Part - 1
A New Mental Model for Acute Care Physicians

By-
Dr Arihant Jain, MD | lifeonthefrontline.com
Instagram: @humans.of.em
X | Linkedin | ORCID
Troponin: 86 ng/L.
The resident looks up and says:
“Sir, the troponin is positive.”

Positive for what?
Acute coronary syndrome?
Myocardial infarction (MI)?
Sepsis-induced myocardial injury?
Chronic kidney disease?
Tachyarrhythmia?
Heart failure?
For decades, we treated troponin as a binary test: positive or negative, infarction or no infarction. High-sensitivity assays have shattered that illusion.
Modern troponin testing has taught us an uncomfortable but essential truth:
Troponin does not diagnose myocardial infarction. Troponin detects myocardial injury.
Everything else requires clinical thinking.
The Great Troponin Misconception
Perhaps the most important contribution of the Fourth Universal Definition of Myocardial Infarction (UDMI) was not a new classification system, but a new vocabulary.
It separated three concepts that clinicians often use interchangeably:
Myocardial injury
Myocardial ischemia
Myocardial infarction
They are not synonymous.
According to the Fourth UDMI, myocardial injury exists whenever cardiac troponin exceeds the 99th percentile upper reference limit (URL) . Myocardial infarction, however, requires much more than an elevated biomarker. It requires evidence that the injury occurred because of ischemia. (Thygesen et al., 2018)
This distinction fundamentally changed cardiovascular medicine.
As Jaffe and colleagues noted, high-sensitivity assays have unmasked the reality that many patients experience myocardial injury in the absence of acute ischemic heart disease (Januzzi et al., 2019).
The challenge for acute care physicians is therefore not simply to recognize an elevated troponin. The challenge is to determine what kind of myocardial injury we are looking at.
The Troponin Triangle: A New Mental Model
Instead of asking:
“Does this patient have an MI?”
We should ask three sequential questions:
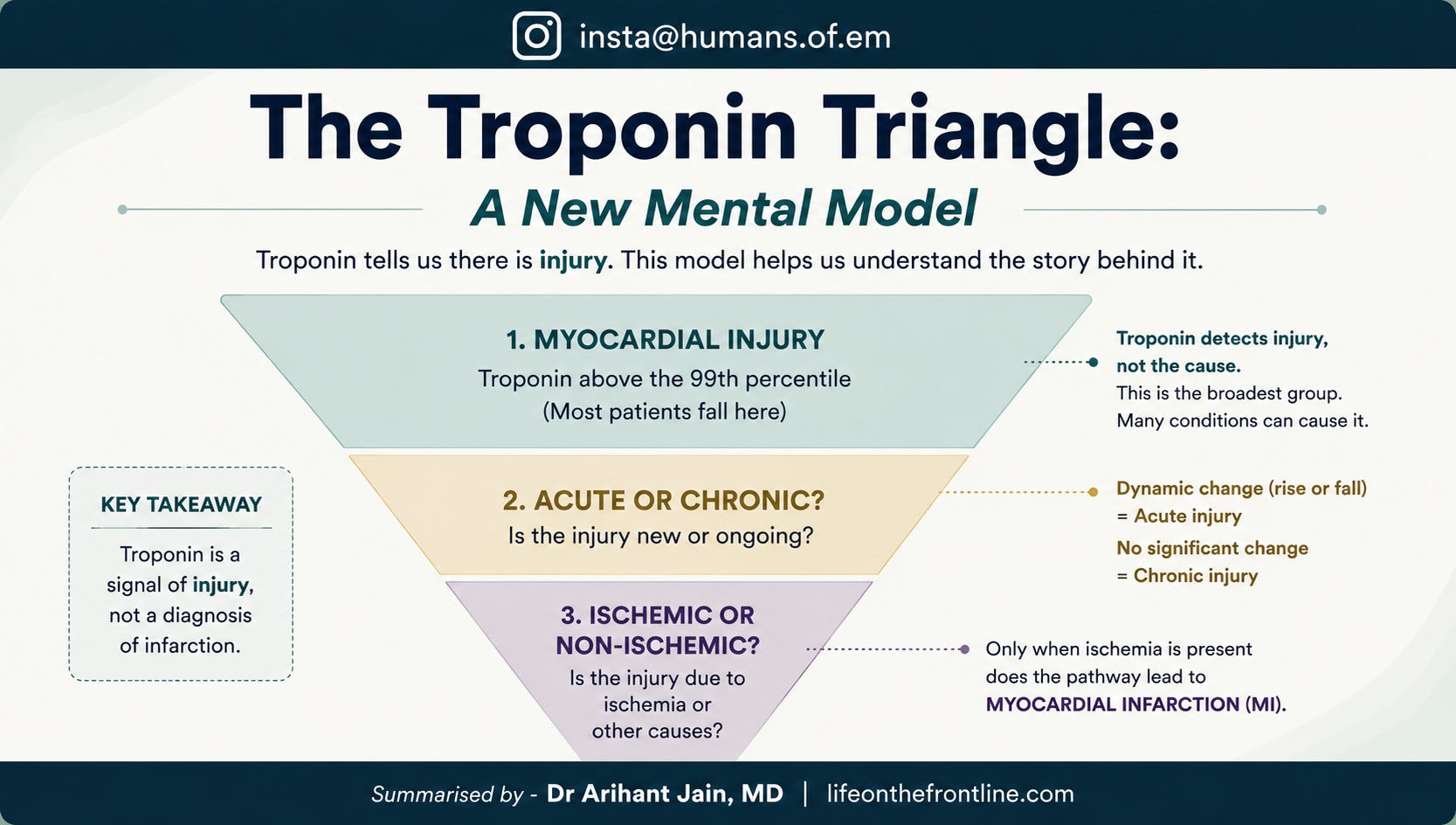
Only one pathway leads to myocardial infarction:
Acute myocardial injury + evidence of ischemia = MI
Everything else remains myocardial injury.
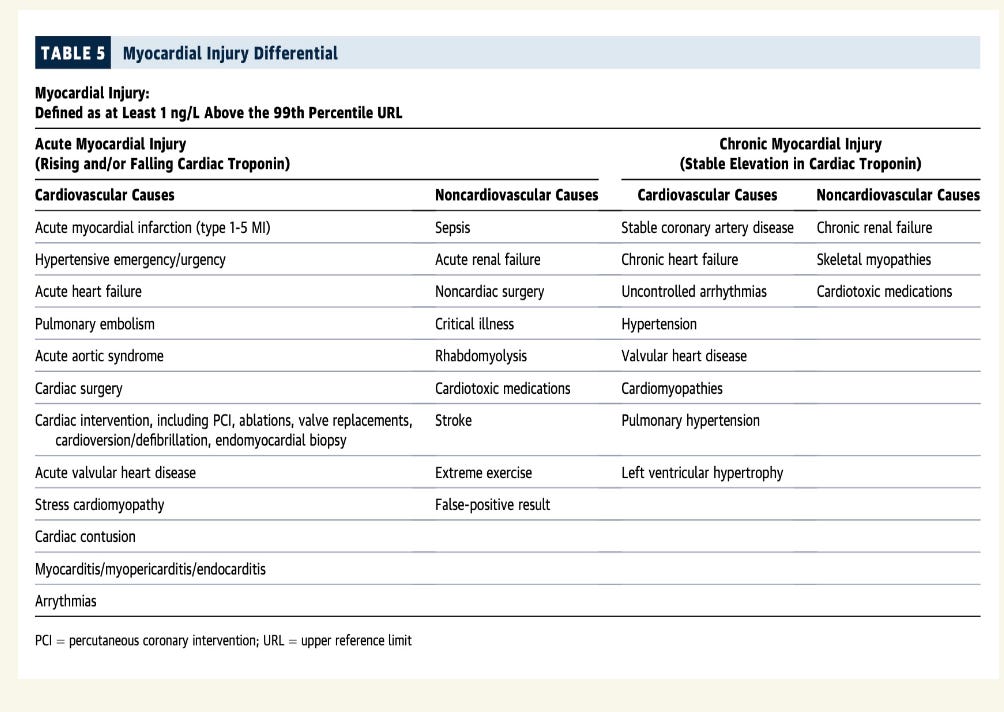
This framework appears deceptively simple, but it immediately clarifies many common diagnostic errors. The patient with septic shock and a rising troponin may have acute myocardial injury.
The patient with CKD and stable troponin elevation may have chronic myocardial injury.
Neither automatically has myocardial infarction. The troponin merely begins the investigation.
Step One:
Is There Myocardial Injury?
The definition is straightforward.
Any cardiac troponin value above the assay-specific 99th percentile URL constitutes myocardial injury (Thygesen et al., 2018).
This 99th percentile URL - is defined for a population and particular assay for both men and women, separately and is specific to the kit.
Not myocardial infarction. Not acute coronary syndrome.
Simply myocardial injury.
High-sensitivity assays now identify extremely small amounts of cardio-myocyte damage that previous generations of tests could never detect (Januzzi et al., 2019).
This increased analytical sensitivity is both a blessing and a burden. It improves early detection of true infarction. But it also reveals how frequently the myocardium suffers injury from non-coronary diseases. The heart, it turns out, is remarkably vulnerable to systemic illness.
The Heart as an Innocent Bystander
Acute care physicians encounter elevated troponin values in almost every critical illness imaginable:
Sepsis
Pulmonary embolism
Stroke
Renal failure
Tachyarrhythmias
Hypertensive emergencies
Acute heart failure
Severe anemia
Carbon monoxide poisoning
Burns
Major trauma
Myocarditis
These conditions injure myocardium. They do not necessarily infarct it. Understanding this distinction is the foundation of modern troponin interpretation.
Step Two:
Is the Injury Acute or Chronic?
This is perhaps the single most under appreciated question in acute care medicine.
The Fourth UDMI defines:
Acute myocardial injury as a rise and/or fall in troponin values.
In contrast:
Chronic myocardial injury refers to persistently elevated but relatively stable troponin concentrations over time (Thygesen et al., 2018).
The number itself matters less than its trajectory.
What Defines Acute Myocardial Injury?
The Fourth Universal Definition states:
Myocardial injury is acute if there is a rise and/or fall in cTn values. (Thygesen et al., 2018)
But it intentionally does not specify a universal numeric cutoff for what constitutes a significant rise or fall. Why?
Because analytical variation differs between assays, and biological variation differs between patients.
Both Rise and Fall Matter
Importantly, both directions are equally significant.
A patient whose troponin changes from:
10 → 30 ng/L has acute myocardial injury.
300 → 180 ng/L also has acute myocardial injury.
The second patient may simply be presenting later in the course of disease, when troponin concentrations are already declining. The myocardium does not care about the direction of the curve.
What matters is that the curve is moving.
A dynamic pattern—whether upward or downward—suggests an active or recently active process, whereas relatively stable values point toward chronic myocardial injury.
Clinical Pearl
Troponin movement matters more than troponin direction.
A patient whose troponin falls from 500 to 300 ng/L may be just as acute as one whose troponin rises from 50 to 250 ng/L. The difference often reflects where the patient sits on the timeline of injury rather than a difference in severity.
Absolute Change vs Percentage Change
This is where modern practice has evolved.
The Current Recommendation
Use ABSOLUTE changes for low or mildly elevated troponin values. Use PERCENTAGE changes only when baseline troponin is substantially elevated.
This is strongly emphasized in modern hs-cTn literature.
Rokos, Mattu, and Jaffe write:
Near the 99th percentile, absolute deltas are statistically superior to relative changes. (Rokos et al., 2025)
Why Absolute Changes Are Better Near the 99th Percentile
Example:
Patient A
Troponin:
10 → 20 ng/L
Absolute change:
+10 ng/L
Relative change:
100%
Clearly significant.
Patient B
Troponin:
500 → 510 ng/L
Absolute change:
+10 ng/L
Relative change:
2%
Probably not clinically meaningful.
Patient C
Troponin:
10 → 12 ng/L
Absolute change:
+2 ng/L
Relative change:
20%
Probably just biological variation. So percentages become misleading at lower concentrations.
This is why:
Modern hs-cTn algorithms prioritize absolute deltas rather than percentage changes.
Practical Rule from the JACC Expert Panel
The JACC Scientific Panel recommends:
If the initial value is near the 99th percentile:
Use absolute change (ng/L).
If the baseline troponin is already substantially elevated (for example, CKD, chronic HF):
A relative change of >20% is often used to suggest superimposed acute injury. This is not perfect science. It is pragmatic bedside medicine.
The famous 20% Rule:
When Should We Use It?
The “20% rule” should be applied carefully.
Appropriate situations:
CKD with chronically elevated troponin.
Chronic heart failure.
Known structural heart disease.
Patients with stable baseline elevations.
Example:
Baseline:
120 ng/L
Repeat:
150 ng/L
Change:
25%
This suggests possible acute-on-chronic injury.
When NOT to use 20%
Do not use percentage changes when:
Values are close to the 99th percentile.
Troponins are in single digits or low double digits.
Using accelerated 0/1-hour or 0/2-hour algorithms.
Absolute values perform better in these situations.
How Much Absolute Change Is Significant?
Unfortunately:
There is no universal number.
It depends entirely on the assay.
Examples from common hs-cTn pathways: (Rokos et al., 2025)
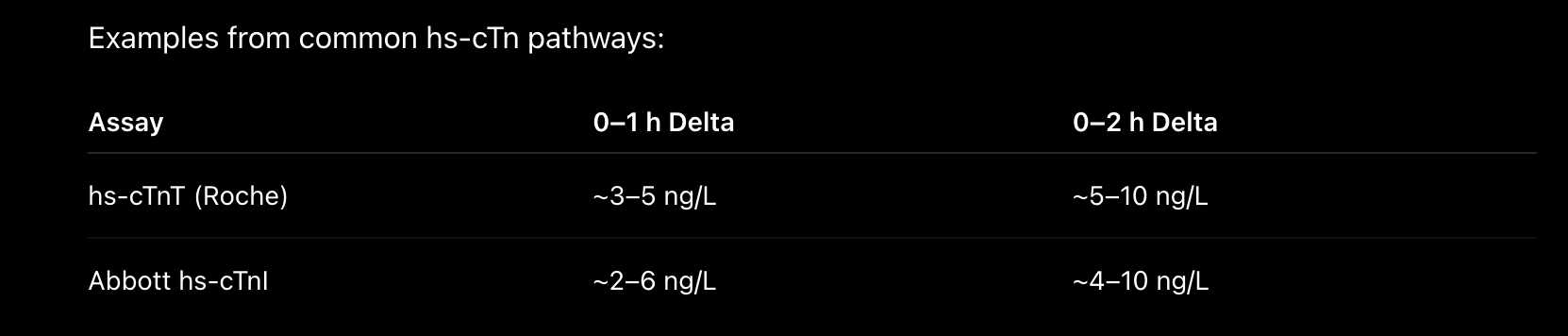
Your hospital must always know:
Which assay is being used.
The assay-specific 99th percentile.
The validated delta thresholds.
There is no “one-size-fits-all” number.
After How Much Time Should We Look for Change?
This is another major shift in the hs-cTn era.
Depends upon the baseline tropI performed for such cases, and the population dynamics where it is validated.
Classical approach
0 hours and 3 hours. ( well validated, can be used in almost all populations)
Modern hs-cTn approach
0–1 hour protocols
Preferred in Europe. Very small absolute changes become meaningful.
0–2 hour protocols
Widely adopted in North America.
Excellent balance between sensitivity and practicality.
3-hour protocols (Only thing useful for INDIA, since others are not validated)
Still useful:
Late presenters.
Resource-limited settings.
When clinical suspicion remains high despite initial testing.

The Most Important Part
Every myocardial infarction causes myocardial injury. But not every myocardial injury is myocardial infarction.
The distinction sounds semantic.
In reality, it changes everything:
Documentation.
Coding.
Prognosis.
Treatment.
Antiplatelet use.
Anticoagulation decisions.
Coronary angiography.
Patient counselling.
Most importantly, it changes how we think.
Coming in Part Two
Once we establish that myocardial injury exists—and determine whether it is acute or chronic—the next question becomes unavoidable:
Is the injury ischemic?
And only then can we discuss:
Type 1 versus Type 2 myocardial infarction.
The modern Trop-Zone approach.
Why the delta often matters more than the absolute number.
The five questions every troponin demands.
A practical bedside algorithm for emergency physicians.
Because in modern acute care:
The elevated troponin is rarely the diagnosis.
It is merely the beginning of the story.
References
Januzzi JL Jr, Mahler SA, Christenson RH, et al. Recommendations for institutions transitioning to high-sensitivity troponin testing. Journal of the American College of Cardiology. 2019;73(9):1059-1077.
Rokos IC, Mattu A, Jaffe AS. High-sensitivity troponin zones: An alternative approach to clinical decisions. The Journal of Emergency Medicine. 2025.
Thygesen K, Alpert JS, Jaffe AS, et al. Fourth universal definition of myocardial infarction (2018). Circulation. 2018;138:e618-e651.
It's really helpful, thank you for sharing 👏🏻