
The Sick Patient Doesn’t Always Look Sick
Rethinking Emergency Department Triage Beyond Physiology

With Insights from :-
Dr Akshay Kumar,
Additional Professor
Department of Emergency Medicine
AIIMS, New Delhi.
The problem with “normal vitals”
A 58-year-old man walks into the ED with chest pain.
Blood pressure? Normal. Oxygen saturation? Normal.

Another patient arrives with unilateral weakness — airway intact, breathing fine.
If we rely only on physiology…
both might wait.
And that’s exactly where triage fails.
Triage is not just numbers
Traditional triage systems often lean heavily on physiology.
But patients don’t present as numbers.
They present as:
Complaints
Patterns
First impressions
Time-sensitive risks
👉 The dangerous truth:
Some of the sickest patients look deceptively stable early (Rauniyar et al., 2025 )
The ATP backbone — necessary, but not sufficient
The AIIMS Triage Protocol (ATP) gives us:
A simple Red–Yellow–Green system
A physiology-first approach
A validated framework in Indian EDs (Singh et al., 2022 )
And it works.
But not completely.
Because:
Early ACS may have normal vitals
Stroke may not trigger physiologic alarms
GI bleed or poisoning may evolve silently
👉 Physiology detects instability — not always risk.
What actually improves triage?
A better model emerges when we stop thinking in silos.
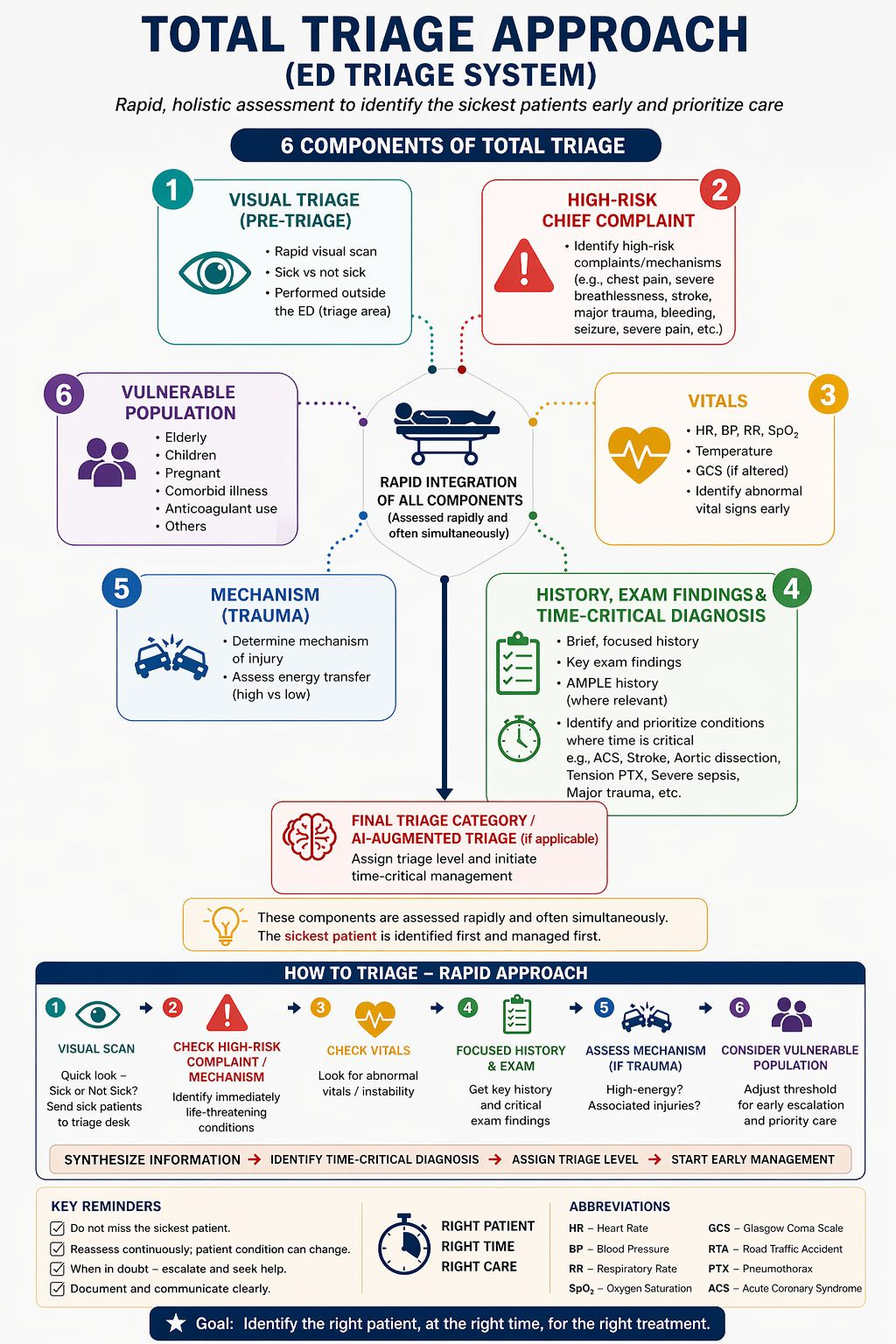
Triage should integrate four simultaneous lenses:
1. Visual impression
“Does this patient look sick?”
Before monitors. Before scores.
Gasping
Seizing
Pale, diaphoretic
“Something is off”
👉 A simple clinical assessment can outperform structured triage in predicting mortality (Iversen et al., 2019 )
2. Physiology (ATP)
Still the backbone.
Airway compromise
Hypoxia
Shock
Low GCS
👉 ATP remains a validated triage framework in LMIC settings (Sahu et al., 2020 )
3. Time-critical diagnoses
Some conditions are dangerous not because of current vitals…
…but because delay kills.
Stroke
Acute coronary syndrome
Major trauma
Sepsis
GI bleed
Poisoning
👉 These are triage diagnoses, not final diagnoses.
But this concept goes beyond traditional medical emergencies.
In many systems, certain conditions are prioritized because early intervention is time-dependent, even when vitals are normal:
Sexual assault survivors (urgent forensic + medical care)
Needle-stick injuries in healthcare workers (time-sensitive prophylaxis)
Testicular or ovarian torsion (time-dependent organ salvage)
👉 These patients may look stable.
👉 Their vitals may be normal.
But delay here is harmful.
Not all Red patients are unstable.
Some are simply time-critical.
4. High-risk chief complaints
Patients arrive with complaints — not diagnoses.
Evidence shows chief complaints independently predict mortality, even after adjusting for vitals (Rice et al., 2020 )
Local AIIMS data further refines this:
Shortness of breath
Altered mental status
Hematemesis
Fall from height
Unilateral weakness
Chest pain
👉 Combining ATP + high-risk complaints
significantly improves predictive accuracy (Rauniyar et al., 2025 )
📌 Follow for more
Dr Arihant Jain, MD
lifeonthefrontline.com
Instagram: @humans.of.em
X - dr__hunt
The integrated triage algorithm
This is the shift:
From single-axis triage → multi-layered triage
⚠️ The most dangerous patient in the ED
Is not the one who is crashing.
It is the one who:
Looks stable
Has “normal vitals”
Is quietly evolving
🤖 Where does AI fit in?
AI is promising — but not ready to replace clinicians.
It may help:
Predict deterioration
Identify hidden risk patterns
Support triage decisions
But current systems face challenges of validation, interpretability, and implementation (Petrella, 2024 )
👉 Triage remains clinician-led.
AI in Emergency Department Triage: What the Research Shows
Artificial intelligence is increasingly being explored to improve triage accuracy, detect deterioration early, and reduce ED burden.
📈 Performance and accuracy
Multiple studies show machine learning models outperform traditional triage systems:
AUROC ~0.82–0.92 vs 0.69–0.80 for standard tools (Raita et al., 2019; Goto et al., 2019; Kang et al., 2020; Yun et al., 2021; Grant et al., 2024)
Improved admission prediction and risk stratification (Hong et al., 2018; Lee et al., 2021)
Advanced models using NLP + multimodal data further enhance prediction and early deterioration detection (Porto, 2024; Choi et al., 2024; Chai et al., 2024)
👉 AI can reduce mis-triage and improve efficiency, though real-world impact remains limited (Abdalhalim et al., 2025; Yi et al., 2024; Kim et al., 2025; Boonstra & Laven, 2022)
🤖 LLMs and chatbot triage
GPT-4 shows high agreement with emergency specialists in controlled settings (Paslı et al., 2024)
But general chatbots show dangerous under-triage rates and are unsafe independently (Halwani et al., 2025; Tortum & Kaşali, 2024)
⚠️ Limitations and risks
Bias, calibration issues, lack of external validation
Over- and under-triage risks
Workflow integration challenges
Explainability concerns
👉 AI is best viewed as decision support, not replacement (Petrella, 2024 ; Porto, 2024; Yi et al., 2024)
Human + AI = the future
AI can:
Improve accuracy
Reduce workload
Support decisions
But triage remains fundamentally clinical, contextual, and human-driven
The takeaway
Use ATP as the backbone.
Upgrade using visual concern, time-critical diagnoses, and high-risk complaints.
Because triage is not a label.
It is a dynamic clinical decision.
Final thought
The question is not:
“What are the vitals?”
The real question is:
“Who should never be allowed to wait?”
References (AMA Style)
Rice B, Leanza J, Mowafi H, et al. Defining high-risk emergency chief complaints: data-driven triage for low- and middle-income countries. Acad Emerg Med. 2020;27:1291–1301.
Petrella RJ. The AI future of emergency medicine. Ann Emerg Med. 2024;84:139–153.
Sahu AK, Bhoi S, Aggarwal P, et al. AIIMS triage protocol (ATP) of a busy ED. J Emerg Trauma Shock. 2020.
Rauniyar N, Sahu AK, Gopinath B, et al. Association of presenting complaint at triage with 72-h mortality and ICU admission. J Emerg Trauma Shock. 2025;18:62–68.
Singh SK, Sahu AK, Kumar A, et al. Prospective validation of a novel triage system developed in a middle-income country—AIIMS triage protocol. J Emerg Trauma Shock. 2022;15:124–127.
Iversen AKS, Kristensen M, Østervig RM, et al. A simple clinical assessment is superior to systematic triage in prediction of mortality in the emergency department. Emerg Med J. 2019;36:66–71.
Raita Y, Goto T, Faridi MK, Brown DFM, Camargo CA Jr, Hasegawa K. Emergency department triage prediction of clinical outcomes using machine learning models. Crit Care. 2019;23:64.
Goto T, Camargo CA Jr, Faridi MK, Freishtat RJ, Hasegawa K. Machine learning–based prediction of clinical outcomes for children during emergency department triage. JAMA Netw Open. 2019;2(1):e186937.
Kang DY, Cho KJ, Kwon O, et al. Artificial intelligence algorithm to predict the need for critical care in prehospital emergency medical services. Scand J Trauma Resusc Emerg Med. 2020;28:17.
Yun H, Choi J, Park J. Prediction of critical care outcomes for adult patients presenting to the emergency department using initial triage information: an XGBoost algorithm analysis. JMIR Med Inform. 2021;9(6):e30770.
Grant L, Diagne M, Aroutiunian R, et al. Machine learning outperforms the Canadian Triage and Acuity Scale (CTAS) in predicting need for early critical care. Can J Emerg Med. 2024;27:43-52.
Hong WS, Haimovich AD, Taylor RA. Predicting hospital admission at emergency department triage using machine learning. PLoS One. 2018;13(7):e0201016.
Lee JH, Hsieh CC, Lin CC, Lin YK, Kao CC. Prediction of hospitalization using artificial intelligence for urgent patients in the emergency department. Sci Rep. 2021;11:98961.
Porto B. Improving triage performance in emergency departments using machine learning and natural language processing: a systematic review. BMC Emerg Med. 2024;24:113.
Choi A, Lee K, Hyun H, et al. A novel deep learning algorithm for real-time prediction of clinical deterioration in the emergency department for a multimodal clinical decision support system. Sci Rep. 2024;14:80268.
Chai C, Peng S, Zhang R, Li C, Zhao Y. Advancing emergency department triage prediction with machine learning to optimize triage for abdominal pain surgery patients. Surg Innov. 2024;31:583-597.
Abdalhalim A, Ahmed S, Ezzelarab A, et al. Clinical impact of artificial intelligence-based triage systems in emergency departments: a systematic review. Cureus. 2025;17:e85667.
Yi N, Baik D, Baek G. The effects of applying artificial intelligence to triage in the emergency department: a systematic review of prospective studies. J Nurs Scholarsh. 2024;57:105-118.
Kim S, Nam S, Lee J. Artificial intelligence in emergency department triage: a scoping review on workload reduction and patient safety enhancement. J Korean Biol Nurs Sci. 2025;25:45.
Boonstra A, Laven M. Influence of artificial intelligence on the work design of emergency department clinicians: a systematic literature review. BMC Health Serv Res. 2022;22:807.
Paslı S, Sahin A, Beşer M, et al. Assessing the precision of artificial intelligence in emergency department triage decisions: insights from a study with ChatGPT. Am J Emerg Med. 2024;78:170-175.
Halwani M, Merdad G, Almasre M, et al. Predicting triage of pediatric patients in the emergency department using machine learning approach. Int J Emerg Med. 2025;18:61.
Tortum F, Kaşali K. Exploring the potential of artificial intelligence models for triage in the emergency department. Postgrad Med. 2024;136:841-846.
Nasser L, McLeod SL, Hall J. Evaluating the reliability of a remote acuity prediction tool in a Canadian academic emergency department. Ann Emerg Med. 2024.
Petrica A, Marza A, Bârsac C, et al. Artificial intelligence in emergency department triage: perspective of human professionals. Front Digit Health. 2026;5:1693060.
Piliuk K, Tomforde S. Artificial intelligence in emergency medicine: a systematic literature review. Int J Med Inform. 2023;180:105274.
I was a triage nurse in A&E, both adults and paediatrics. The main thing we did was to listen to the patient or parent whilst observing them. Sudden onset of chest pain described as sharp following strenuous activity, exacerbated by breathing, although observations are within range, patient speaking in full sentences. On auscultation reduced breath sounds on the right upper chest area. I suspected pneumothorax, verified by X ray.
Patient attends with tachycardia and fever, has been unwell for 24 hours with fever. Need to rule out/rule in sepsis as the priority.
For children the most important information is going to come from the parents as they know their child better than we do.