
The Heart Failure Syndrome
Not All Heart Failure Is the Same — And Not All of It Needs Lasix

In the emergency department, heart failure often triggers muscle memory.
Oxygen.
IV access.
And almost reflexively—Lasix.
But heart failure is not a single disease, and congestion is not universal.
Treating all heart failure the same way is one of the quieter cognitive errors we make—not from ignorance, but from habit.
Emergency medicine and acute care demands something harder:
Phenotype recognition before therapy and POCUS can help
Heart Failure Is a Syndrome, Not a Protocol
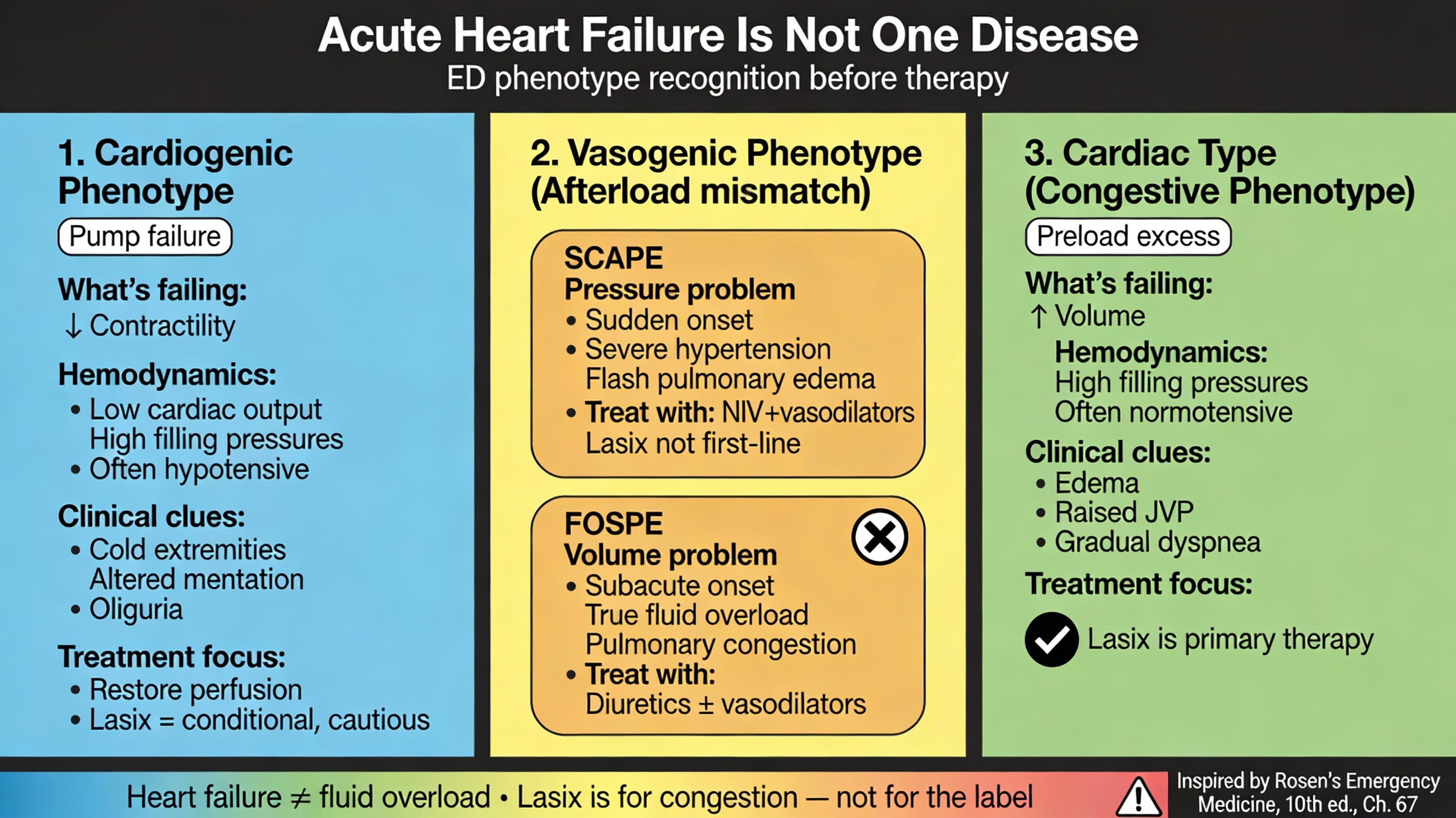
As emphasized in Rosen’s Emergency Medicine - 10th Edition, acute heart failure in the ED does not represent one uniform pathophysiology. Instead, it presents as distinct hemodynamic phenotypes, each driven by a different dominant failure—of pump, pipes, or preload (Chapter 67).
Recognizing what is actually failing determines what helps—and what harms.
The Three ED-Relevant Heart Failure Phenotypes
1️⃣ Cardiogenic Phenotype
Primary problem: Pump failure (reduced contractility)
Physiology
Low cardiac output
Elevated filling pressures
Often hypotension or narrow pulse pressure
Clinical clues
Cold extremities
Altered mentation
Oliguria
Hypoperfusion with or without congestion
ED implication
This is true cardiogenic physiology.
Aggressive vasodilation or reflex diuresis without hemodynamic assessment can precipitate collapse.
Lasix is not automatic here—it is conditional, cautious, and secondary to restoring perfusion.
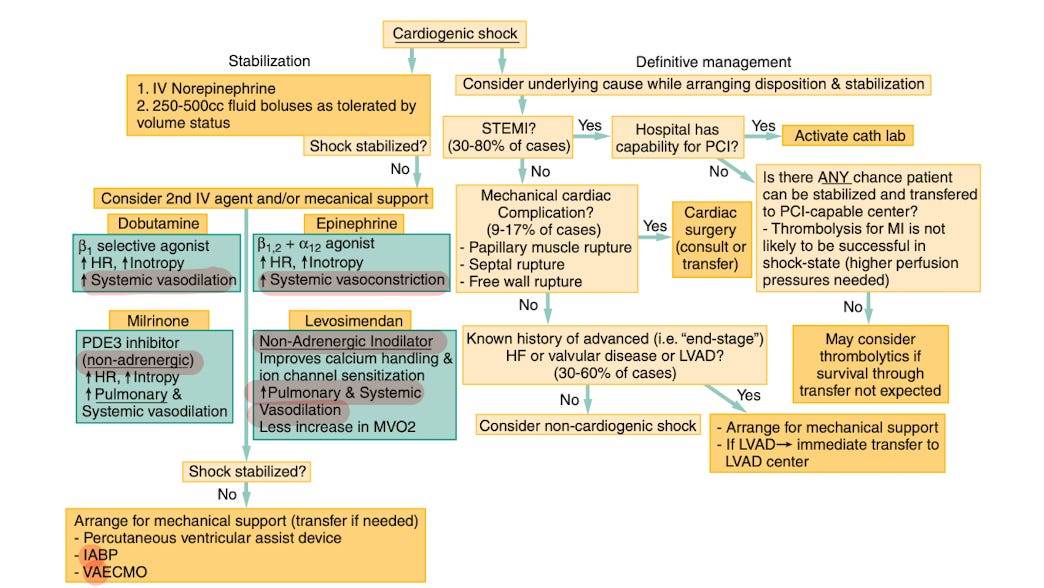
Image taken from fig 67.13 _ Rosen’s 10th edition
Treatment Include - Stabilisation of shock hemodynamics and considering underlying cause ( ?ACS or other acute events)
(Felker et al., 2020; Rosen’s EM, 10th ed., Ch. 67)
2️⃣ Vasogenic Phenotype (Afterload Mismatch)
Primary problem: Excessive systemic vascular resistance
Contractility: Often preserved
Blood pressure: Hypertensive to patient’s baseline
This phenotype is frequently mistaken for “fluid overload,” when the dominant problem is actually afterload.
Two important ED subtypes:
a. SCAPE — Sympathetic Crashing Acute Pulmonary Edema
Abrupt onset (minutes to hours)
Marked hypertension
Severe respiratory distress
Flash pulmonary edema
Warm peripheries
Physiology
A sudden sympathetic surge causes a dramatic rise in SVR, forcing a relatively normal ventricle to fail against pressure—without true volume excess.
ED implication
Rapid vasodilation - NTG bolus and high dose infusion. (IBCC _ SCAPE chapter/ emcrit.org)
Early noninvasive ventilation —> HFNC —> Intubation.
Diuretics are not first-line in the initial phase
b. FOSPE — Fluid Overload Subacute Pulmonary Edema
Gradual onset (hours to days)
True volume overload , similar to cardiac - congestive phenotype
Often hypertensive, but less extreme than SCAPE, have afterload problems too
Pulmonary congestion with systemic fluid excess plus increased afterload.
Physiology
Progressive salt and water retention increases preload, eventually overwhelming the pulmonary circulation—sometimes with a secondary afterload component.
ED implication
NTG low dose infusion (If HTN to patient’s baseline) - no role of NTG bolus
f/b diuretics - Diuretics have a clear role
Early noninvasive ventilation —> HFNC —> Intubation.
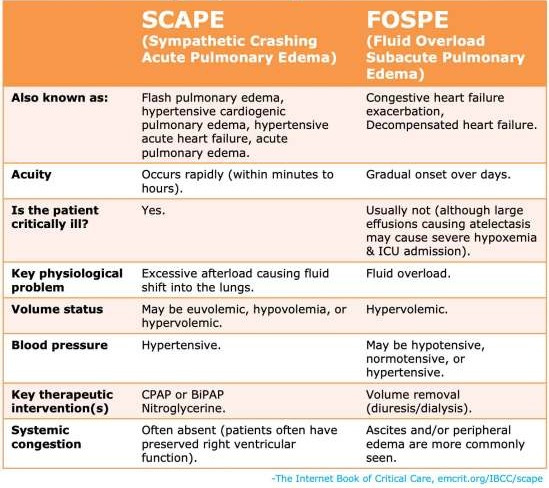
A Critical Distinction
SCAPE fails because of pressure.
FOSPE fails because of volume.
Confusing the two delays improvement—and occasionally causes harm.
Use POCUS as an adjunct to differentiate
(Mullens et al., 2019; Rosen’s EM, Ch. 67)
3️⃣ Cardiac Type (Congestive / Volume-Overload–Dominant)
Primary problem: Excess preload and normal BP.
Physiology
Elevated filling pressures
Variable cardiac output
Often normotensive
Clinical clues
Peripheral edema
Raised JVP
Hepatic congestion
Gradual symptom progression
ED implication
This is the phenotype where loop diuretics clearly help.
Here, Lasix is treatment—not tradition.
(Bilgeri et al., 2024; Palazzuoli et al., 2024)
The Lasix Fallacy
Guidelines and position statements are consistent on one point:
Loop diuretics are recommended for acute heart failure with clinical congestion, not for every patient labeled “HF.”
The Heart Failure Association of the European Society of Cardiology explicitly frames its guidance as “diuretics in heart failure with congestion” (Mullens et al., 2019).
Contemporary reviews reinforce that diuretic use must be individualized according to phenotype, volume status, renal interaction, and trajectory—not diagnosis alone (Palazzuoli et al., 2024).
Observational ED data show that a substantial proportion of patients admitted with heart failure receive no IV diuretics, often because they are euvolemic or presenting with a non-congestive phenotype—without worse outcomes (Qadri et al., 2022).
Heart failure does not equal fluid overload.
The danger is not in giving Lasix—
it is in giving it without understanding why.
And in emergency medicine and acute care, why is often the difference between improvement and deterioration.
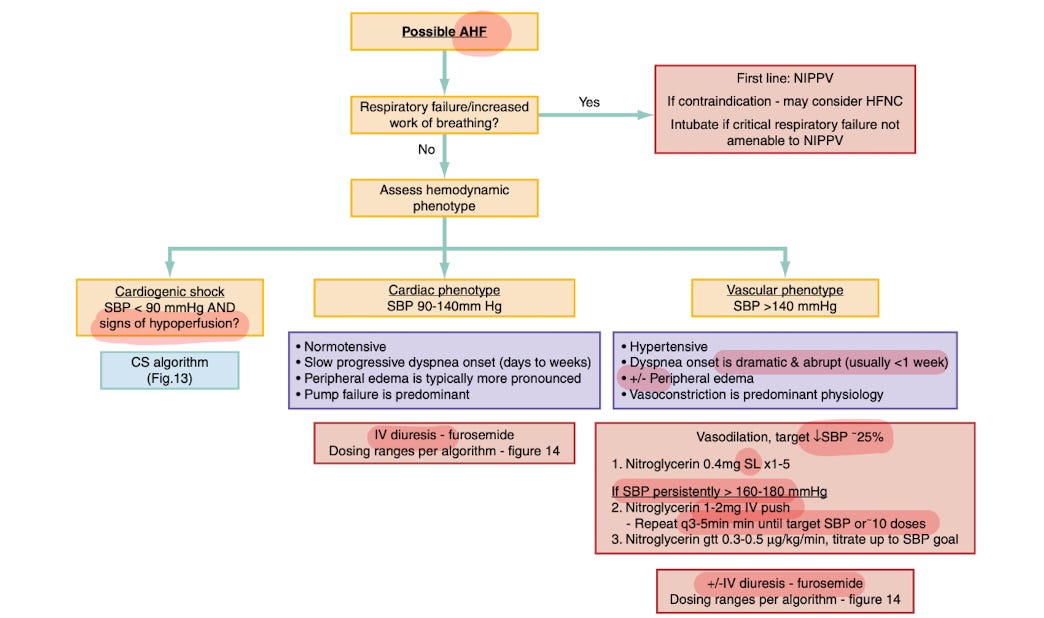
Image taken from Rosen’s 10th Edition. Chapter 67.
A Better ED Question
Instead of asking:
“Does this patient have heart failure?”
Ask:
Which failure is dominant right now—cardiogenic, vasogenic (SCAPE or FOSPE), or cardiac-congestive?
Only one phenotype reliably needs Lasix upfront.
Use POCUS to differentiate.
REFERENCES -
Walls RM, Hockberger RS, Gausche-Hill M, eds. Rosen’s Emergency Medicine: Concepts and Clinical Practice. 10th ed. Chapter 67. Elsevier; 2022.
Mullens W, Damman K, Harjola VP, et al. The use of diuretics in heart failure with congestion: a position statement from the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail. 2019;21(2):137-155. doi:10.1002/ejhf.1369
Felker GM, Ellison DH, Mullens W, Cox ZL, Testani JM. Diuretic therapy for patients with heart failure: a JACC state-of-the-art review. J Am Coll Cardiol. 2020;75(10):1178-1195. doi:10.1016/j.jacc.2019.12.059
Farkas JD. Sympathetic crashing acute pulmonary edema (SCAPE). In: Internet Book of Critical Care (IBCC). EMCrit Project. Published online. Accessed 2026. https://emcrit.org/ibcc/scape/
Bilgeri V, Spitaler P, Puelacher C, Messner M, et al. Decongestion in acute heart failure—time to rethink and standardize current clinical practice. J Clin Med. 2024;13(2):311. doi:10.3390/jcm13020311
Palazzuoli A, Mazzeo P, Fortunato M, Dessalvi CC, et al. The changing role of loop diuretics in heart failure management across the last century. J Clin Med. 2024;13(6):1674. doi:10.3390/jcm13061674
Qadri N, Thomas C, Madrid S, Rush P, Strauss C, Bradley SM. Diuretic use in the emergency department and outcomes in patients hospitalized with heart failure. Circ Cardiovasc Qual Outcomes. 2022;15(suppl 1):A183. doi:10.1161/CIRCOUTCOMES.15.suppl_1.183
Absolutely loved this phenotype-first framing. In the ED, “heart failure” too often becomes a reflex label that triggers a reflex treatment, when the physiology is telling us to pause and ask what is failing right now: pump, pipes (afterload), or preload. That one shift in question can be the difference between rapid improvement and iatrogenic worsening. 
The SCAPE vs FOSPE distinction is especially high-yield: SCAPE is fundamentally pressure/afterload mismatch with abrupt sympathetic surge, where early aggressive vasodilation + noninvasive ventilation can be life-saving, and diuretics are often not the first move. FOSPE and the more classic congestive phenotype are the scenarios where loop diuretics reliably help because volume excess is truly driving the presentation. 
Also appreciate the practical call-out: “Lasix is not wrong; Lasix without a why is the problem.” POCUS as an adjunct (LV function, IVC, B-lines, pleural effusions) plus a quick hemodynamic gestalt (warm/cold, wet/dry, BP phenotype) makes this approach doable even on busy shifts. 
This is the kind of post that improves care tomorrow morning; thank you for putting language and structure around a common cognitive error!
Is FOSPE same as the cardiac - congestive phenotype variant?