
The art of Anti-Platelet therapy
Updated with the 2026 ACC Scientific Statement: How modern anti-platelet therapy should change your approach to ACS, stroke, and peri-operative care ?

"The first physician to see the patient often makes the decision that matters the most."
By-
Dr Arihant Jain, MD | lifeonthefrontline.com
Instagram: @humans.of.em
X | Linkedin | ORCID
——————————————————————————————————————
It’s 2:17 a.m.
A 58-year-old man arrives clutching his chest. The ECG leaves little room for doubt, an anterior STEMI. While the cath lab is being activated, the nurse turns to you.
“Doctor, which anti-platelet should I load?”
Before you’ve answered, another patient rolls in. A 72-year-old woman with a minor ischemic stroke, well within 4.5 hours of symptom onset.
Should she receive aspirin alone? Or dual anti-platelet therapy? or nothing at all?
As you’re reviewing her CT, the surgical registrar calls.
“We’ve got a patient with a perforated bowel. He’s on aspirin and ticagrelor after a stent placed three months ago. Can we stop them?”
Three patients. Three anti-platelet decisions. Three completely different answers.
Yet every one of them starts with the same question.
Why is this patient need an anti-platelet?
Not which drug. Not how long they’ve been taking it. But why?
‘If this article helped simplify a difficult bedside decision, consider sharing it with your ED or acute care team, leave your thoughts in the comments, and subscribe to Life on the Frontline for more practical, evidence-based guides from the world of emergency and acute care.’
Because modern anti-platelet therapy is no longer about memorizing drugs. It’s about understanding the balance between thrombosis and bleeding, and recognizing that this balance changes with time (Kumbhani et al., 2026).
In the ED, we are often the first physicians to influence that balance. We decide what gets loaded, what gets withheld, what should continue before surgery, and what should never be stopped. This article isn’t a cardiology review.
It’s a practical guide to the anti-platelet decisions emergency and acute care physicians make every shift.
A Mental Model Before We Begin
Whenever you encounter a patient on anti-platelets, pause and ask three questions.
1. Why was it started?
Acute coronary syndrome?
PCI?
Stroke?
Peripheral arterial disease?
Primary prevention?
2. How recent was the event?
Hours? Days? Weeks? Years?
A patient one week after PCI is very different from one who had a stent placed five years ago.
3. What is the biggest threat today?
Bleeding? Or thrombosis?
Everything else follows from these three questions.
Decision 1
Which Anti-platelet Should I Load in the Emergency Department?
This is probably the most common and one of the most important antiplatelet decisions we make.
The answer depends entirely on where the patient is going next.
Primary PCI?
Fibrinolysis?
Early invasive NSTEMI?
Conservative management?
Each pathway has a different strategy.
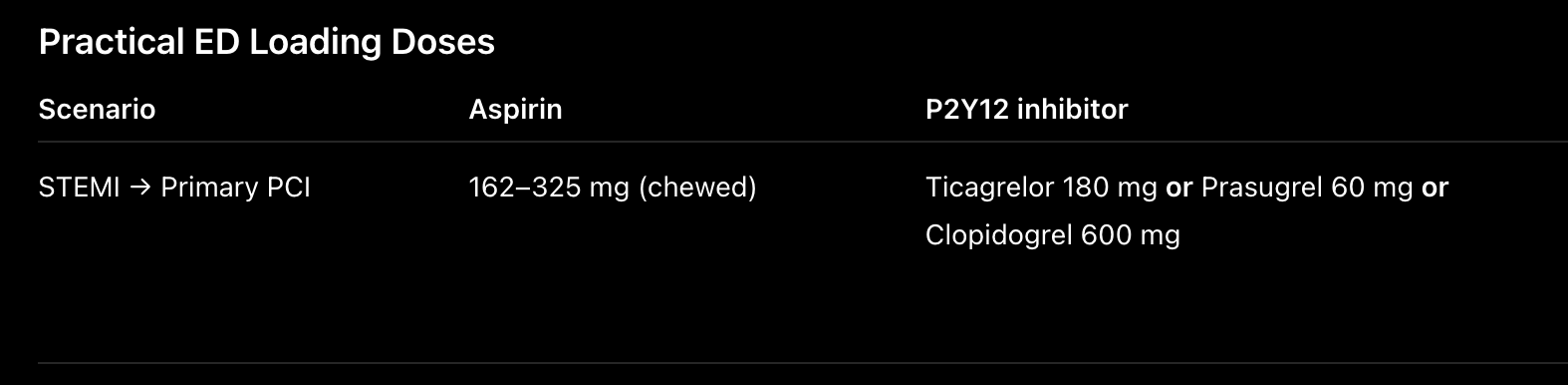
Scenario 1: STEMI Going for Primary PCI
Imagine you’re in the resuscitation bay. The ECG shows a large anterior STEMI. The cath lab has accepted the patient. Your priority is simple:
Achieve rapid and potent platelet inhibition before coronary instrumentation.
The current standard is:
Chewed aspirin 162–325 mg
Plus a P2Y12 inhibitor
For most patients undergoing primary PCI, ticagrelor or prasugrel are preferred over clopidogrel because they produce faster, more potent, and more predictable platelet inhibition, reducing ischemic events and stent thrombosis (Wallentin et al., 2009; Wiviott et al., 2007; Kumbhani et al., 2026).
Which P2Y12 Inhibitor Should I Choose?
Ticagrelor
Ticagrelor has become the default choice in many emergency departments. Why?
Rapid onset
No metabolic activation required
Potent platelet inhibition
Reversible receptor binding
The PLATO trial demonstrated lower cardiovascular mortality compared with clopidogrel without increasing overall major bleeding, making it an attractive first-line agent in ACS (Wallentin et al., 2009).
Prasugrel
Prasugrel is equally potent and in PCI-treated patients may even outperform ticagrelor in selected populations (Schüpke et al., 2019).
However, remember its major limitations. Avoid prasugrel in patients with:
Previous stroke or TIA
Age ≥75 years (unless benefits clearly outweigh risks)
Weight <60 kg
Unlike ticagrelor, many operators prefer administering prasugrel after coronary anatomy has been defined, particularly if there is a realistic possibility the patient will require CABG.
Clopidogrel
Clopidogrel still has an important place. It remains reasonable when:
Ticagrelor or prasugrel are unavailable
Bleeding risk is high
Cost is a major issue
Potent P2Y12 inhibitors are contraindicated
Think of clopidogrel not as an “inferior” drug—but as the right drug for selected patients.
Frontline Pearl
PCI favors potent platelet inhibition. If the patient is heading to the cath lab, think ticagrelor or prasugrel first.
Scenario 2: STEMI Receiving Thrombolysis
Now imagine a different hospital. No PCI capability. Transfer will take four hours. The patient is receiving tenecteplase. Should you still load Ticagrelor or Prasugrel?
No.
This is one of the most common misconceptions among junior doctors. The evidence supporting fibrinolysis was built around clopidogrel, not the newer P2Y12 inhibitors.
Recommended Strategy
Why Not Ticagrelor?
Could ticagrelor work? Possibly.
Should it replace clopidogrel routinely with thrombolysis? Not yet.
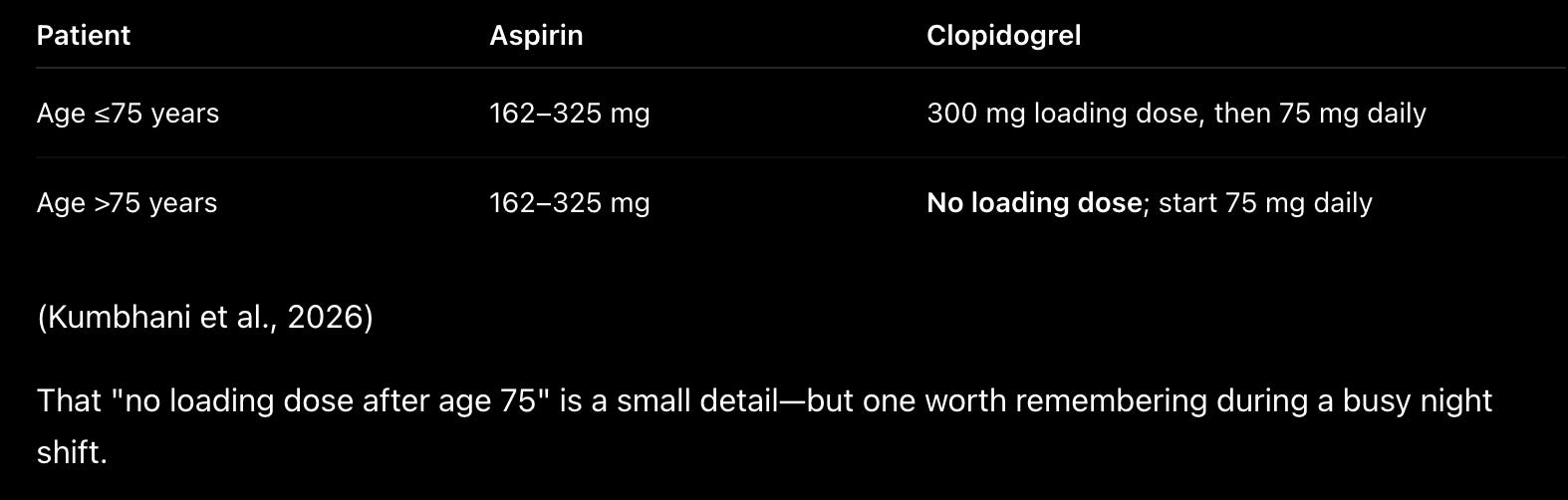
The strongest evidence for pharmaco-invasive STEMI still supports aspirin plus clopidogrel after fibrinolysis, and contemporary guidelines continue to recommend this approach (Kumbhani et al., 2026).
Scenario 3: NSTE-ACS
Very High Risk or High Risk NSTE- ACS , continue same approach as of STEMI requiring PCI.
but for others,
This is where things become less straightforward. For years, many of us loaded clopidogrel as soon as we diagnosed NSTEMI. That practice has changed.
Modern evidence suggests routine pretreatment before coronary anatomy is known offers little benefit and may complicate patients who ultimately require CABG (Kumbhani et al., 2026).
My Practical Approach
If early angiography (<24 hours) is planned:
Give aspirin.
Discuss P2Y12 timing with cardiology.
In many patients, defer loading until coronary anatomy is defined.
If angiography will be delayed or the patient is managed conservatively:
Loading with ticagrelor or clopidogrel when appropriate is reasonable.
Common ED Pitfalls
❌ Giving prasugrel to a patient with previous stroke.
❌ Loading ticagrelor in a patient receiving thrombolysis because “it’s newer.”
❌ Automatically loading every NSTEMI before discussing the invasive strategy.
❌ Forgetting that patients over 75 years receiving fibrinolysis do not receive a clopidogrel loading dose.
Decision 2
Does Every ACS Patient Still Need 12 Months of Dual Anti-platelet Therapy?
For years, the answer was simple. Every patient with ACS received 12 months of dual antiplatelet therapy (DAPT)—usually aspirin plus a P2Y12 inhibitor.
It was easy to remember. It was also easy to teach. But like many “rules” in medicine, it turned out to be only partly true. Over the past decade, improvements in stent technology, PCI techniques, and the availability of more potent anti-platelet agents have fundamentally changed the conversation. Today’s question is no longer:
“Should every patient receive 12 months of DAPT?”
Instead, we ask:
“How long does this particular patient need protection from thrombosis before the risk of bleeding becomes the greater threat?”
That shift—from fixed-duration therapy to individualized therapy—is perhaps the biggest conceptual change in modern anti-platelet management (Kumbhani et al., 2026).
The first month after an ACS is a dangerous time. Platelets are highly activated. The stent is still endothelializing. The culprit plaque remains biologically unstable.
This is precisely when dual antiplatelet therapy (DAPT) provides its greatest benefit. But as weeks turn into months, something interesting happens—the risk of stent thrombosis falls rapidly, while the cumulative risk of bleeding continues to rise.
That’s why modern antiplatelet therapy is no longer about one duration for everyone. It is about matching the duration of DAPT to the patient’s evolving balance between ischemic and bleeding risk (Kumbhani et al., 2026).
The New Way to Think About DAPT
Instead of asking:
“Should I stop DAPT at 12 months?”
Ask:
“Has the patient’s bleeding risk now become greater than their ischemic risk?”
If the answer is yes, shortening DAPT may be safer. If the answer is no, prolonged therapy may still provide benefit.
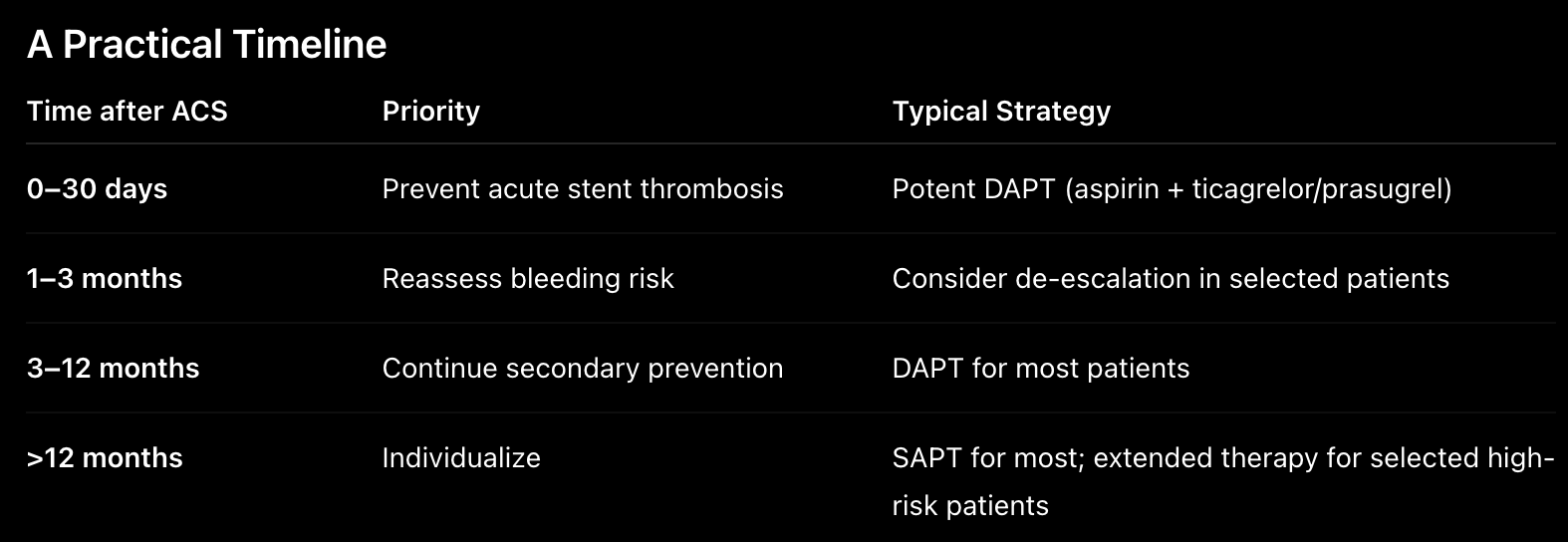
When Can We Shorten DAPT?
Several contemporary trials have shown that selected patients can safely transition to P2Y12 inhibitor monotherapy after 1–3 months of DAPT, reducing bleeding without a significant increase in ischemic events (Mehran et al., 2019; Valgimigli et al., 2021).
Who should you think about?
Older adults
Previous GI bleeding
Chronic kidney disease
Frailty
Need for future surgery
Concurrent anticoagulation
De-escalation: Less Can Be More
Imagine your patient returns three months after PCI. No recurrent ischemia. Now they develop upper GI bleeding.
Do they still need potent DAPT? Maybe not.
In carefully selected patients, switching from ticagrelor or prasugrel to clopidogrel, or stopping aspirin and continuing a P2Y12 inhibitor alone, can substantially reduce bleeding while maintaining acceptable ischemic protection (Kumbhani et al., 2026).
Decision 3
The Patient Has an Acute Ischemic Stroke. Should I Give Aspirin, Dual Antiplatelet Therapy, or Neither?
A 69-year-old man presents 90 minutes after sudden right arm weakness and aphasia. His CT brain shows no hemorrhage.
Before you think about aspirin or clopidogrel, ask yourself one question:
Is this patient a candidate for reperfusion therapy?
This is arguably the most important antiplatelet decision in acute stroke care. Giving anti-platelets too early in a patient proceeding for intravenous thrombolysis or mechanical thrombectomy can increase bleeding risk without improving outcomes.
Step 1: Is the Patient Eligible for Reperfusion?
Intravenous thrombolysis
Eligible?
Do NOT administer aspirin or any P2Y12 inhibitor before thrombolysis.
Following alteplase or tenecteplase, all antiplatelet and anticoagulant therapy should be withheld for the first 24 hours.
A repeat CT (or MRI) demonstrating no intracranial hemorrhage is required before initiating antiplatelet therapy (Powers et al., 2019; European Stroke Organisation, 2023).
Mechanical thrombectomy
Patients proceeding directly for thrombectomy without thrombolysis similarly should not receive routine antiplatelet loading before reperfusion, unless there is another specific indication (such as emergent intracranial stenting).
Once post-procedure imaging excludes hemorrhage, antiplatelet therapy can be started according to the underlying stroke mechanism and procedural findings.
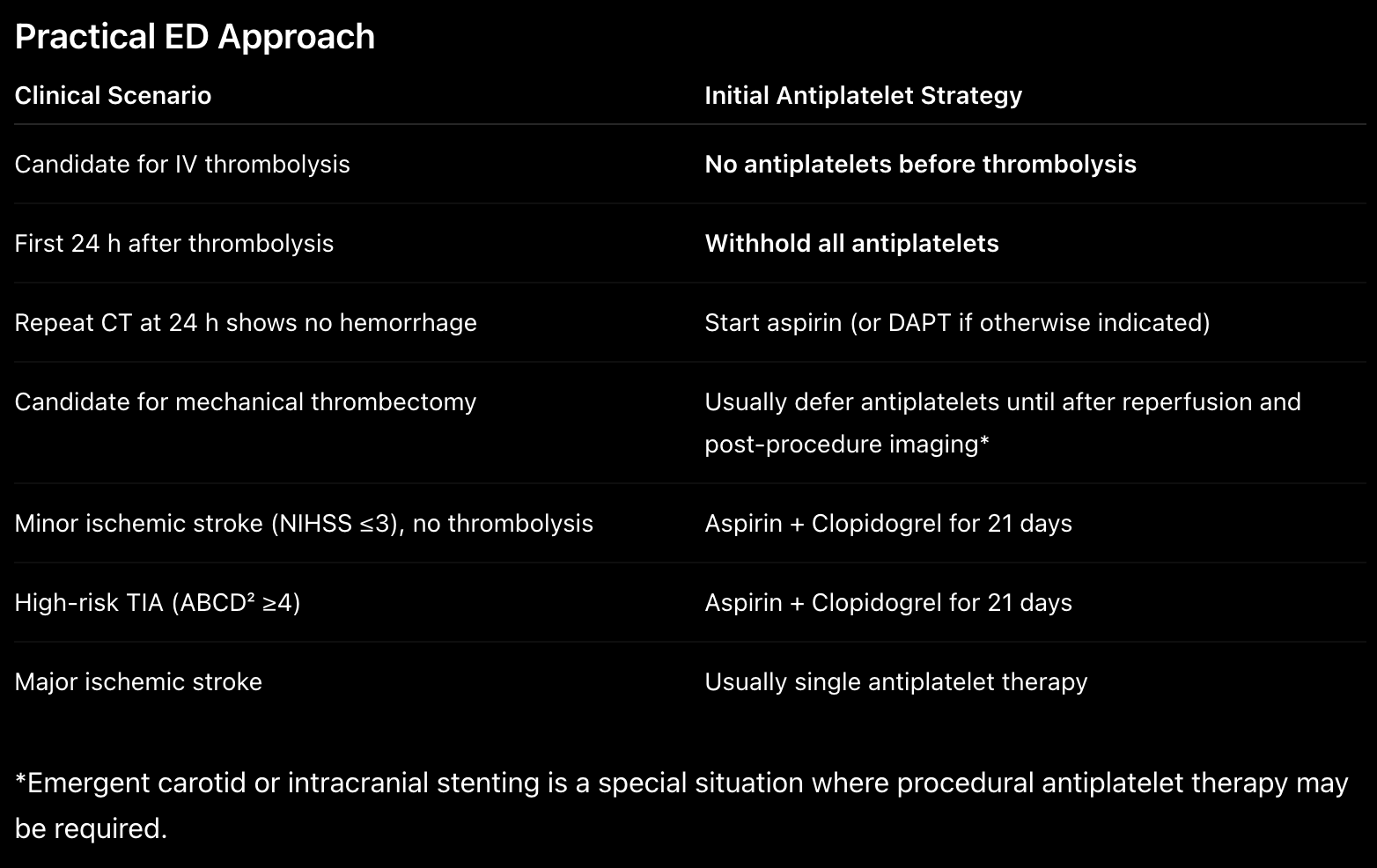
(Kumbhani et al., 2026)
Minor Stroke: Aspirin Alone or Dual Antiplatelet Therapy?
A 69-year-old man presents with sudden right arm weakness that resolved within 20 minutes. His CT brain is normal. He has a National Institutes of Health Stroke Scale (NIHSS) score of 1.
Should he receive aspirin? Or dual antiplatelet therapy? The answer depends on stroke severity.
Minor Stroke and High-Risk TIA
Three landmark trials—CHANCE, POINT, and THALES—changed our practice. For patients with:
Minor ischemic stroke (NIHSS ≤3)
High-risk TIA (ABCD² ≥4)
Early initiation of DAPT reduces recurrent stroke, particularly during the first three weeks (Wang et al., 2013; Johnston et al., 2018).
Why Only 21 Days?
Because recurrent stroke risk is highest immediately after the event. After three weeks, the incremental benefit of DAPT diminishes, while bleeding risk continues to increase. Unlike ACS, where DAPT is measured in months, stroke DAPT is measured in weeks. (Kumbhani et al., 2026)
Decision 4
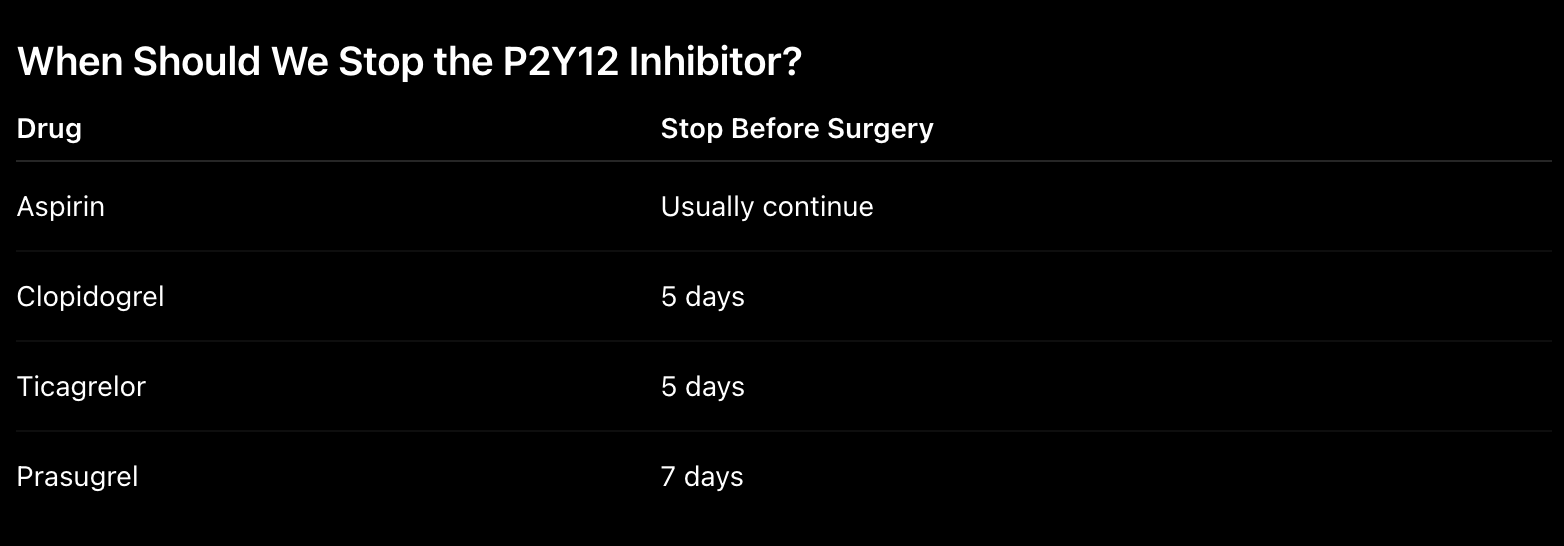
The Surgeon Wants to Stop the Anti-platelets
Few phone calls create more anxiety than this one.
“Doctor, can we stop the aspirin before surgery?”
The answer isn’t simply yes or no. It depends on why the patient is taking it. A patient taking aspirin for primary prevention is very different from one who underwent PCI six weeks ago.
Elective Surgery After PCI
Whenever possible:
Delay surgery at least 6 months after PCI for chronic coronary disease.
Delay surgery 12 months after PCI for ACS.
(Kumbhani et al., 2026)
Emergency Surgery
Sometimes surgery simply cannot wait.
Options include:
Proceeding despite antiplatelet therapy when delay would be more dangerous.
Platelet transfusion in selected life-threatening bleeding scenarios.
Bridging with intravenous cangrelor in carefully selected recent PCI patients.
(Kumbhani et al., 2026)
Decision 5
The Patient Is Already Taking a DOAC
An 80-year-old patient with atrial fibrillation undergoes PCI.
Should you prescribe:
Aspirin + Clopidogrel + Apixaban?
That used to be standard practice. Today, prolonged triple therapy has largely disappeared.
Modern Strategy
For most patients:
Short course of triple therapy (1–4 weeks)
Then discontinue aspirin
Continue DOAC + clopidogrel
This strategy substantially reduces bleeding while preserving ischemic protection (Kumbhani et al., 2026).
Final Thoughts
Antiplatelet therapy has become far more nuanced than it was a decade ago. Yet the bedside approach remains surprisingly simple. Understand why the therapy was started. Recognize how the patient’s risk changes with time. And remember that the best antiplatelet strategy is rarely the most aggressive one—it is the one that strikes the right balance between preventing thrombosis and avoiding harm.
As emergency and acute care physicians, we are often the first to make that decision. It may be as simple as choosing the correct loading dose in a STEMI, or as difficult as deciding whether to stop DAPT before emergency surgery. Either way, our decisions shape what happens long after the patient leaves the Emergency Department.
References
Kumbhani DJ, Gibson CM, Kinlay S, et al. Antiplatelet Therapy in the Management of Atherosclerotic Cardiovascular Disease: 2026 ACC Scientific Statement. J Am Coll Cardiol. 2026.
Wallentin L, Becker RC, Budaj A, et al. Ticagrelor versus clopidogrel in patients with acute coronary syndromes. N Engl J Med. 2009.
Wiviott SD, Braunwald E, McCabe CH, et al. Prasugrel versus clopidogrel in ACS undergoing PCI. N Engl J Med. 2007.
Schüpke S, Neumann FJ, Menichelli M, et al. Ticagrelor or prasugrel in patients with acute coronary syndromes. N Engl J Med. 2019.
Mehran R, Baber U, Sharma SK, et al. Ticagrelor with or without aspirin after PCI (TWILIGHT). N Engl J Med. 2019.
Valgimigli M, Frigoli E, Heg D, et al. Dual antiplatelet therapy after PCI in high bleeding risk patients (MASTER DAPT). N Engl J Med. 2021.
Wang Y, Wang Y, Zhao X, et al. Clopidogrel with aspirin in acute minor stroke or TIA (CHANCE). N Engl J Med. 2013.
Johnston SC, Easton JD, Farrant M, et al. Clopidogrel and aspirin in acute ischemic stroke and high-risk TIA (POINT). N Engl J Med. 2018.