
The Acute Pulmonary Embolism, Part 1: Classification and Diagnosis
The 2026 AHA/ACC/ACEP physiology-based classification (A–E groups), : applying the new A–E framework in ED decision-making

Pulmonary embolism is one of the most feared diagnoses in emergency medicine.
Not because it is rare—but because it is unpredictable.
Some patients with PE are discharged safely from the emergency department within hours. Others arrest suddenly despite appearing stable minutes earlier.
The difference is not clot size.

It is physiology of clot against RV.
The 2026 AHA/ACC Pulmonary Embolism guideline replaces the outdated “massive vs submassive vs low-risk” terminology with a dynamic, physiology-based classification system (Groups A–E) that integrates clinical severity scores, biomarkers, RV imaging, hemodynamics, and respiratory status.
This framework begins in the emergency department—at the moment of diagnosis—and directly determines prognosis, monitoring, disposition, and treatment.
This article focuses on definition, classification, evaluation, and diagnosis—from the emergency department.
Definition of Acute Pulmonary Embolism
Acute pulmonary embolism is defined as:
Obstruction of pulmonary arterial circulation by thrombus, resulting in impaired pulmonary perfusion, increased pulmonary vascular resistance, and potential right ventricular (RV) failure.
The clinical consequences depend on the interaction between:
• Clot burden
• Speed of vascular obstruction
• RV reserve
• Cardiopulmonary reserve
• Systemic compensation
The right ventricle—not the clot—is the primary determinant of outcome.
Epidemiology: The ED Reality
Pulmonary embolism presents a paradox in emergency medicine.
It is common—but rarely confirmed.
Key ED statistics:
• Only 4–10% of patients undergoing CTPA for suspected PE actually have PE
• Acceptable diagnostic miss rate: <2% at 3 months
• Age-adjusted D-dimer diagnostic strategy failure rate: 0.3% (95% CI 0.1–1.7%)
• DVT is present in 44–71% of confirmed PE patients
This defines the core emergency medicine challenge:
Identify dangerous PE while safely excluding PE in the majority.
The New AHA/ACC/ACEP Classification (A–E)
The 2026 guideline introduces a five-group classification system reflecting progressive physiological severity.
Each group directly correlates with mortality risk, disposition, and treatment escalation.
GROUP A: Subclinical (Incidental) PE
Definition:
Pulmonary embolism detected incidentally on imaging, without attributable symptoms.
These patients have no physiological compromise.
Mortality risk: <1%
Subgroups
A1: Subsegmental incidental PE
Features:
• Isolated subsegmental embolus
• No symptoms
• No RV dysfunction
• No hypoxia
• Normal biomarkers
Physiology intact.
Lowest-risk group.
A2: Segmental or proximal incidental PE
Features:
• Larger clot burden
• Still asymptomatic
• Normal hemodynamics
• No RV dysfunction
Anatomical clot present—but physiological compensation intact.
GROUP B: Symptomatic PE, Low Clinical Severity
Definition:
Symptomatic PE with low severity scores:
• PESI Class I–II
• sPESI = 0
• Hestia negative
RV function preserved.
Mortality risk: ~1%
Subgroups
B1: Symptomatic sub-segmental PE
Features:
• Symptoms present
• Minimal clot burden
• Normal RV function
• Normal biomarkers
B2: Symptomatic segmental or proximal PE
Features:
• Larger clot burden
• Symptoms present
• RV function preserved
• Hemodynamically stable
These represent compensated pulmonary embolism physiology.
Many can be safely treated as outpatients.
GROUP C: Symptomatic PE with Elevated Clinical Severity
RV injury present, but no shock
Definition:
Symptomatic PE with elevated clinical severity scores:
• PESI Class III–V
• sPESI ≥1
• Hestia positive
• Bova score ≥4
Represents early RV dysfunction.
Mortality risk increases progressively across subgroups.
Subgroups
C1: Elevated clinical severity score only
Features:
• Elevated PESI/sPESI
• Normal RV function
• Normal troponin
• Normal BNP
Risk driven by co-morbid vulnerability.
Mortality risk: ~3–5%
C2: RV dysfunction OR biomarker elevation
Features:
Either:
• RV dilation on imaging
OR
• Elevated troponin or BNP
Indicates early RV myocardial stress.
Mortality risk: ~5–15%
C3: RV dysfunction AND biomarker elevation
Features:
• RV dilation present
• Elevated troponin
• Elevated BNP
Represents established RV injury.
Blood pressure still preserved due to compensation.
Mortality risk: 15–30%
This is the highest-risk normotensive subgroup.
Equivalent to old ‘Intermediate - High Risk Group’
Respiratory Modifier: “R”
Any subgroup may receive a respiratory modifier (R) if respiratory failure present.
Examples:
C3R
D2R
E1R
Defined by:
• Oxygen requirement ≥6 L/min
• Non-invasive ventilation
• Mechanical ventilation
Pulm Embolism new guidelines
This identifies patients at risk of respiratory collapse independent of hypotension.
GROUP D: Incipient Cardiopulmonary Failure
Shock physiology emerging
Most important group to identify
These patients demonstrate circulatory compromise without persistent hypotension.
Mortality risk: 20–40%
Subgroups
D1: Transient hypotension
Features:
• Temporary hypotension
• Responds to fluids
• No persistent organ hypoperfusion
Represents unstable compensation.
D2: Normotensive shock
Features:
• SBP ≥90 mmHg
• Lactate ≥2 mmol/L
• Evidence of organ hypoperfusion
Shock present despite preserved blood pressure.
Extremely high risk.
GROUP E: Cardiopulmonary Failure
Established shock or cardiac arrest
Highest-risk group.
Mortality risk: >40%
Pulm Embolism new guidelines
Subgroups
E1: Cardiogenic shock
Features:
• Persistent hypotension
• Vasopressor requirement
• RV failure present
E2: Refractory shock or cardiac arrest
Features:
• Persistent shock despite therapy
• Cardiac arrest
Highest mortality subgroup.
Emergency Department Diagnostic Approach (COR and LOE)
The guideline recommends a structured, stepwise approach.
Step 1: Clinical Assessment
COR 1, LOE A
Pulm Embolism new guidelines
Includes:
Symptoms:
• Dyspnea
• Chest pain
• Syncope
• Hemoptysis
Signs:
• Tachycardia
• Hypoxia
• Hypotension
• Signs of DVT
Risk factors:
• Prior VTE
• Surgery
• Immobilization
• Cancer
• Pregnancy
Step 2: Clinical Probability Assessment
COR 1, LOE A
Pulm Embolism new guidelines
Validated tools:
• Wells Score
• Revised Geneva Score
• PERC Rule
These determine need for testing.
Step 3: D-Dimer Testing
COR 2a, LOE B-R
Pulm Embolism new guidelines
Indicated in low or intermediate probability patients.
Age-adjusted D-dimer improves diagnostic efficiency.
Failure rate: 0.3%
Step 4: Imaging with CTPA
COR 1, LOE A
Pulm Embolism new guidelines
CTPA is diagnostic standard.
Advantages:
• High sensitivity and specificity
• Rapid diagnosis
• RV assessment
• Alternative diagnoses identified
Step 5: RV Assessment and Biomarkers
COR 1, LOE B-R
Pulm Embolism new guidelines
Critical prognostic parameters include:
• RV/LV ratio ≥1.0
• Troponin elevation
• BNP elevation
• TAPSE <1.6 cm
These identify RV dysfunction.
Echocardiographic Findings in Acute PE: Sensitivity, Specificity, and Likelihood Ratios
Important guideline principle:
The AHA/ACC guideline emphasizes that echo should NOT be used to rule out PE (COR 3 – No Benefit), but is strongly recommended for risk stratification and identification of RV dysfunction (COR 1, LOE B-NR).
Pulm Embolism new guidelines
Single findings have limited sensitivity.
Multiple findings greatly increase diagnostic probability.
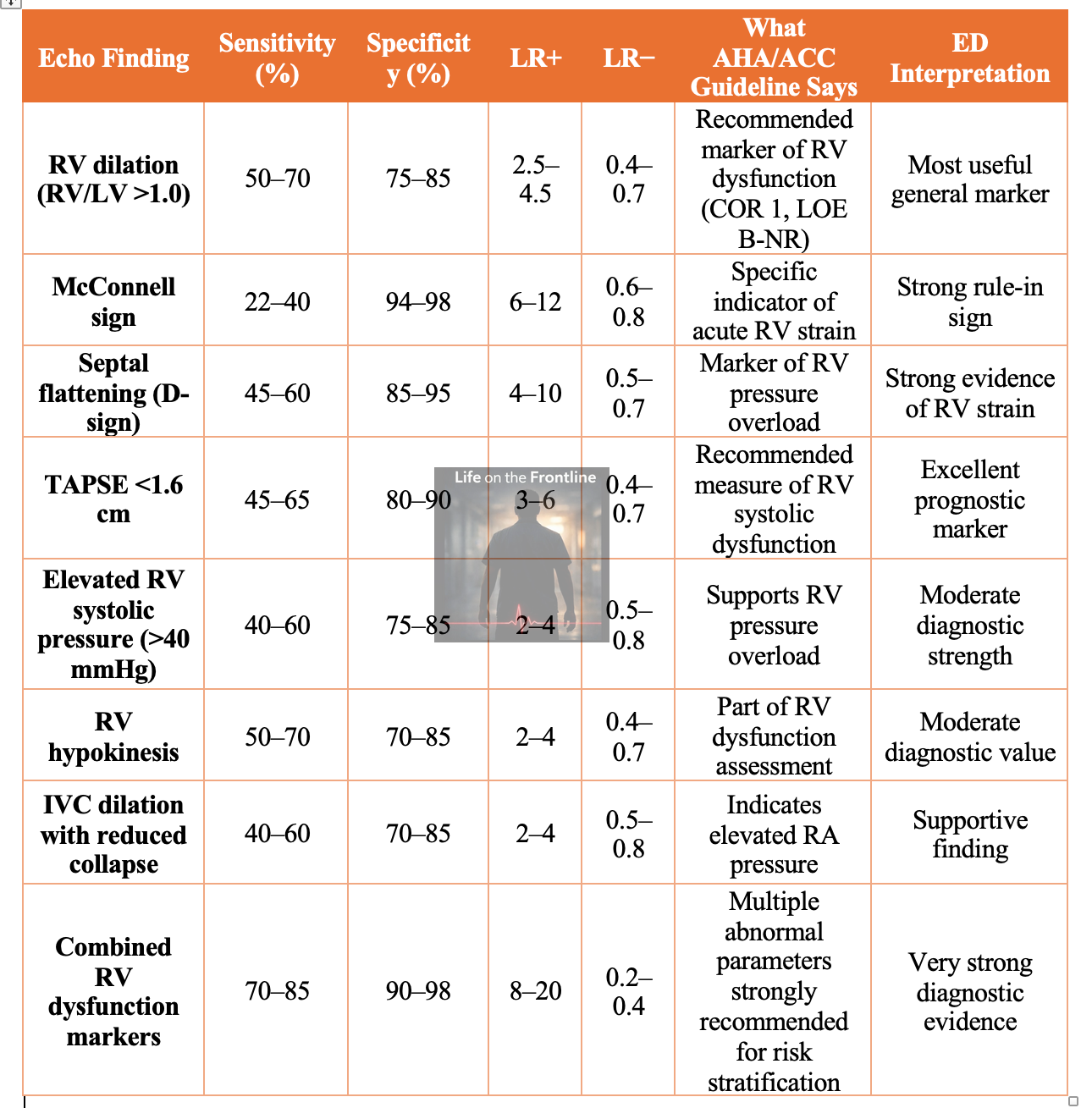
Highest-Value Echo Findings Ranked by Likelihood Ratio
From strongest to weakest diagnostic strength:
McConnell sign → LR+ up to 12
Septal flattening → LR+ up to 10
Multiple RV dysfunction markers → LR+ up to 20
TAPSE <1.6 cm → LR+ up to 6
RV dilation → LR+ up to 4
Guideline-Specific Key Recommendations on POCUS/Echo (COR and LOE)
POCUS for diagnosis
COR 3 (No Benefit), LOE B-NR
Echo should not be used alone to diagnose or exclude PE.
Reason: poor sensitivity.
Cardiac POCUS for risk stratification
COR 1, LOE B-NR
Echo is recommended to assess RV dysfunction and risk.
Pulm Embolism new guidelines
Multiple parameters improve accuracy
Guideline explicitly states:
Sensitivity and specificity improve significantly when multiple RV dysfunction parameters are present.
Pulm Embolism new guidelines
Emergency Medicine Interpretation Algorithm Using Likelihood Ratios
Pretest probability determines how POCUS (Cardiac) findings affect diagnosis.
Example: Moderate probability patient
Pretest probability: 30%
McConnell sign present
LR+ = 10
Post-test probability → ~80–90%
Strongly supports PE diagnosis and high-risk physiology.
Example: Echo normal
LR− ~0.6
Post-test probability drops modestly.
Cannot exclude PE.
CTPA still required.
Most Important ED Clinical Insight
POCUS is not sensitive enough to exclude PE.
highly valuable for identifying dangerous PE.
identifies physiology—not clot.
answers the question:
Is the right ventricle failing?
Not:
Is there a clot?
Highest-Yield Bedside Rule for Emergency Physicians
Presence of ≥2 of the following strongly supports acute PE with RV strain:
• RV dilation
• McConnell sign
• Septal flattening
• TAPSE <1.6 cm
• Elevated RVSP
Post-test probability becomes very high.
Why Classification Matters in the Emergency Department
This classification determines:
• Who can be discharged
• Who requires admission
• Who requires ICU care
• Who requires reperfusion therapy
This decision begins in the emergency department.
Not after admission.
Critical Emergency Medicine Insight
The most dangerous PE is not the hypotensive patient.
It is the normotensive patient with failing RV physiology.
The new A–E classification allows emergency physicians to identify these patients before collapse occurs.
This is the true purpose of classification.
New Insights: Update on diagnosis of hemo-dynamically unstable patient - unstable to shift to CTPA
In hemodynamically unstable patients where computed tomography pulmonary angiography (CTPA) is unsafe or impossible, multi-organ point-of-care ultrasound (POCUS)—combining focused cardiac, lung, and lower limb venous assessment—can support a working diagnosis of pulmonary embolism and guide urgent reperfusion decisions, although it cannot definitively exclude PE.
Focused cardiac ultrasound primarily evaluates for acute right ventricular (RV) pressure overload, with key findings including RV dilation (RV/LV ratio >1), septal flattening (“D-sign”), reduced TAPSE, tricuspid regurgitation, and McConnell’s sign, which demonstrates high specificity (~98.6%) but low sensitivity (~29%) for acute PE (Fields et al., 2017; Falster et al., 2021; Oh & Park, 2023).
Lung ultrasound may identify peripheral pleural-based wedge-shaped infarcts with sensitivity of approximately 80–81% and specificity of 87%, supporting the diagnosis in the appropriate clinical context (Falster et al., 2021; Du et al., 2024; Mohamed et al., 2023). Compression ultrasound demonstrating proximal deep venous thrombosis is highly specific (96–97%) and, when combined with shock and RV strain, strongly supports PE as the cause of hemodynamic instability (Dwyer et al., 2017; Falster et al., 2021).
Importantly, multiorgan POCUS protocols significantly improve diagnostic performance compared with single-organ assessment, achieving sensitivity up to 90% and specificity ranging from 69–86% in critically ill populations (Girardi et al., 2022; Lieveld et al., 2022; Melo et al., 2025).
In unstable patients with high clinical probability and concordant POCUS findings—particularly RV strain with or without confirmed DVT—current evidence supports initiating anticoagulation or thrombolysis when alternative causes of shock have been reasonably excluded (Falster et al., 2021; Oh & Park, 2023).
If you found this useful, follow for more visual emergency medicine breakdowns.
I regularly share clinical algorithms, airway physiology, and critical care insights on Instagram:
→ @humans.of.em
More visual explainers and ED-focused pearls are posted there.
Coming Next: Part 2
Part 2 will cover:
• Anticoagulation selection
• Thrombolysis and thrombectomy indications
• ICU vs ward vs discharge decisions
• Monitoring and escalation
• Complications including CTEPH
• Follow-up strategies
All mapped directly to A–E classification.
References
American College of Cardiology/American Heart Association Joint Committee. 2026 AHA/ACC guideline for the diagnosis and management of acute pulmonary embolism. J Am Coll Cardiol. 2026.
Fields JM, Davis J, Girson L, et al. Transthoracic echocardiography for diagnosing pulmonary embolism: a systematic review and meta-analysis. J Am Soc Echocardiogr. 2017;30(7):714-723.e4. doi:10.1016/j.echo.2017.03.004
Falster C, Jacobsen N, Coman KE, et al. Diagnostic accuracy of focused deep venous, lung, cardiac and multiorgan ultrasound in suspected pulmonary embolism: a systematic review and meta-analysis. Thorax. 2021;77(7):679-689. doi:10.1136/thoraxjnl-2021-216838
Girardi AM, Turra E, Loreto M, et al. Diagnostic accuracy of multiorgan point-of-care ultrasound compared with pulmonary CT angiography in critically ill patients with suspected pulmonary embolism. PLoS One. 2022;17(10):e0276202. doi:10.1371/journal.pone.0276202
Mohamed H, Farouk N, Elnaeem E, et al. Sensitivity and specificity of chest ultrasound in the diagnosis of pulmonary embolism in the emergency department. Can J Respir Ther. 2023;59:123-129. doi:10.29390/cjrt-2022-065
Dwyer KH, Rempell JS, Stone MB. Diagnosing centrally located pulmonary embolisms in the emergency department using point-of-care ultrasound. Am J Emerg Med. 2017;36(7):1145-1150. doi:10.1016/j.ajem.2017.11.033
Melo RB, Gioli-Pereira L, Lourenço I, et al. Diagnostic accuracy of multi-organ point-of-care ultrasound for pulmonary embolism in critically ill patients: a systematic review and meta-analysis. Crit Care. 2025;29:59. doi:10.1186/s13054-025-05359-x
Lieveld AWE, Heldeweg MLA, Smit JM, et al. Multi-organ point-of-care ultrasound for detection of pulmonary embolism in critically ill patients. J Crit Care. 2022;69:153992. doi:10.1016/j.jcrc.2022.153992
Fantastic read is there a podcast on this as well? Would love to hear it.
Excellent updating. Thanks