The 2026 Dyslipidemia Guideline: From Numbers to Lifelong Risk
How the new ACC/AHA update reshapes LDL targets, risk tools, and young‑MI prevention for acute and general physicians

Why should an ED or ICU doctor care about a lipid guideline?
You are stabilising a 34‑year‑old STEMI at 3 a.m. or admitting a 45‑year‑old with necrotising pancreatitis and triglycerides of 1400 mg/dL.
In those moments, dyslipidemia can feel like someone else’s follow‑up problem. The 2026 ACC/AHA Dyslipidemia Guideline is a polite but firm reminder that it is your problem too.
This guideline replaces the 2018 “blood cholesterol” document and expands the focus to LDL‑C, triglycerides, and lipoprotein(a), with an explicit goal: reduce lifelong exposure to atherogenic lipoproteins and prevent recurrent events. For acute care physicians, this means aligning in‑hospital decisions with long‑term targets rather than leaving lipids to vague outpatient plans.
Big picture: what actually changed?
Three shifts matter in acute care:
From “current LDL” to “lifetime exposure”
The guideline emphasizes early lifestyle and pharmacologic treatment in youth and young adults, especially those with familial hypercholesterolemia (FH) or LDL‑C ≥160 mg/dL with strong family history of premature ASCVD. The rationale is simple: event risk in the ED often reflects decades of cumulative LDL burden.From Pooled Cohort Equations to PREVENT
For adults 30–79 years with LDL‑C 70–189 mg/dL and no clinical or subclinical ASCVD, the PREVENT‑ASCVD equations replace the Pooled Cohort Equations for 10‑ and 30‑year risk estimation. Categories are:Low: <3%
Borderline: 3–<5%
Intermediate: 5–<10%
High: ≥10% 10‑year risk.
As an acute physician, you may not open a calculator mid‑resus, but you should know that risk tools have changed and now explicitly incorporate 30‑year risk for 30–59‑year‑olds.
From “start a statin” to “hit a target”
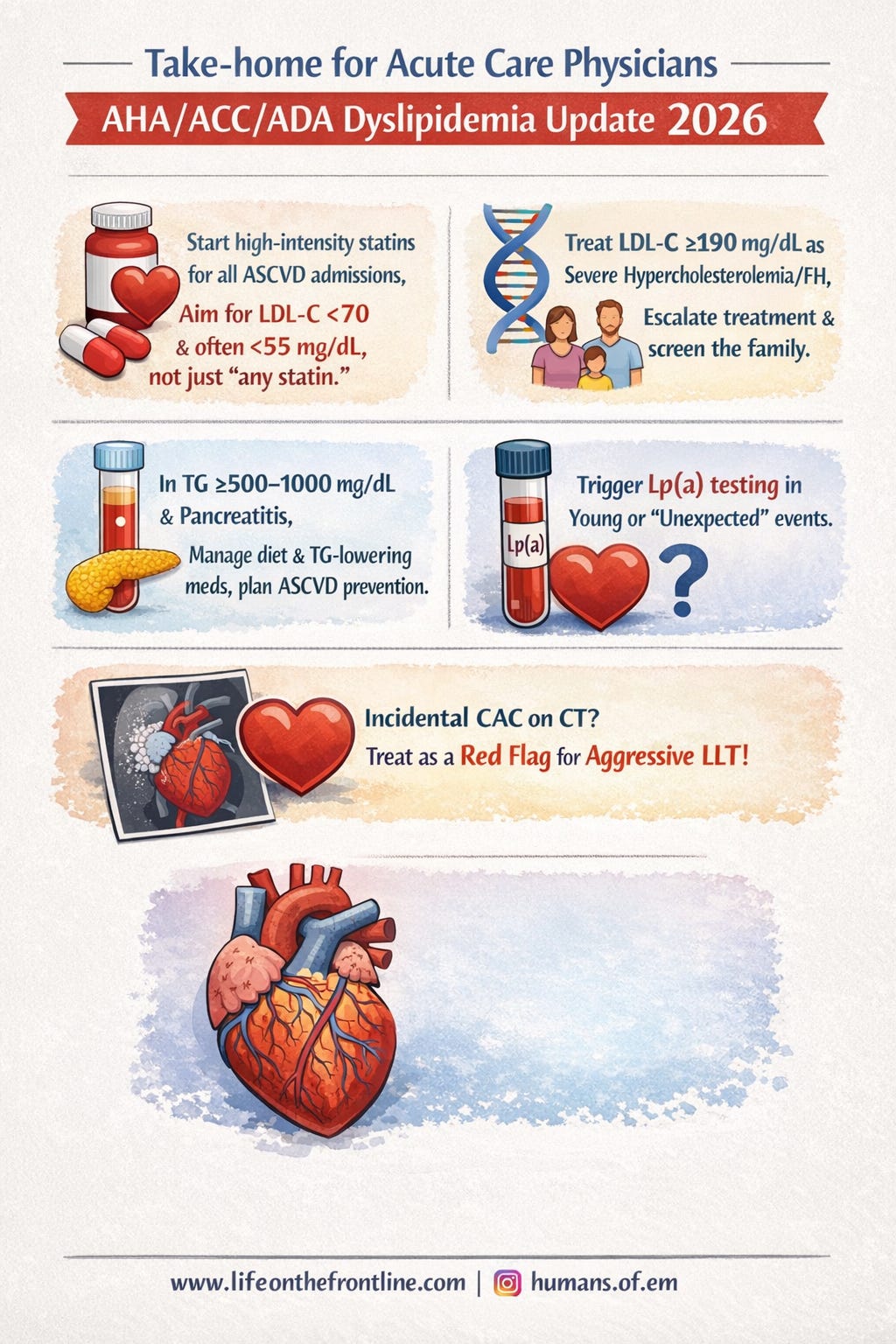
LDL‑C and non‑HDL‑C goals are back. Secondary prevention and high‑risk groups now have targets like LDL‑C <70 mg/dL for all ASCVD and <55 mg/dL for very‑high‑risk or heavy CAC. Your discharge prescriptions should be written with these numbers in mind.
In the ED and ICU: what should you actually do?
1. Treat every ACS as a lipid intervention opportunity
For any patient with clinical ASCVD (ACS, prior MI, stroke, PAD):
Start or escalate to high‑intensity statin (e.g., atorvastatin 40–80 mg, rosuvastatin 20–40 mg) during the index admission unless contraindicated.
The goal in “standard‑risk” ASCVD is:
≥50% reduction in LDL‑C, and
LDL‑C <70 mg/dL with non‑HDL‑C <100 mg/dL (Class I).
For very high‑risk ASCVD (e.g., multiple events, multivessel coronary disease, diabetes plus ASCVD):
The recommended goal is:
LDL‑C <55 mg/dL and non‑HDL‑C <85 mg/dL.
If your patient is already on a high‑intensity statin and clearly above these targets, document the need to add ezetimibe and/or a PCSK9 monoclonal antibody as soon as feasible (Class IIa).
Your role: make sure high‑intensity statin is started, contraindications are documented, and the discharge summary explicitly states the LDL‑C target and the need to escalate if it is not met.
2. Recognise severe hypercholesterolemia and FH in young MI
In a 30‑ or 40‑year‑old with MI:
If LDL‑C is ≥190 mg/dL, this is severe hypercholesterolemia and often FH.
The guideline recommends:
High‑intensity statin as a baseline.
For those without ASCVD, additional non‑statins (ezetimibe, PCSK9 mAb, bempedoic acid) to reach LDL‑C <100 mg/dL and non‑HDL‑C <130 mg/dL are Class I.
If there is clinical ASCVD or confirmed HeFH/high CAC, targets tighten to LDL‑C <70 or <55 mg/dL depending on risk, with combination therapy recommended.
Your role: identify these patients early, flag possible FH, and ensure the team plans family screening and multi‑drug therapy rather than “MI at 35, statin alone”.
3. Manage hypertriglyceridemia to prevent pancreatitis and later events
For patients presenting with severe hypertriglyceridemia, especially with pancreatitis:
TG ≥1000 mg/dL:
Very low‑fat diet, restricted refined carbohydrates, complete elimination of alcohol and added sugars, plus referral to a registered dietitian nutritionist are Class I recommendations to lower TG and prevent pancreatitis.
In familial chylomicronemia syndrome with TG ≥1000 mg/dL, olezarsen (apoC3 inhibitor) is recommended as adjunct to diet to reduce pancreatitis risk (Class I).
TG 500–999 mg/dL:
Similar aggressive lifestyle measures plus pharmacologic TG‑lowering (fibrates or omega‑3 ethyl esters), tailored to clinical context.
Once the acute phase is controlled, statins remain the backbone of long‑term ASCVD risk reduction in these patients.
Your role: in pancreatitis and severe hyperTG, act decisively in the first 24–48 hours on diet, secondary causes, and TG‑lowering therapy, and then ensure a plan to start/intensify statins is documented for follow‑up.
4. Use admissions to trigger Lp(a) and future risk workup
The guideline recommends measuring lipoprotein(a) once in all adults for ASCVD risk assessment (Class I).
For emergency/hospital physicians, practical opportunities include:
Young or “unexpected” MI or stroke.
Patients with premature ASCVD in multiple family members.
Recurrent events despite “acceptable” LDL‑C.
Elevated Lp(a) (≥125 nmol/L or ≥50 mg/dL) is a risk‑enhancing factor associated with ~1.4‑fold higher ASCVD risk; ≥250 nmol/L or ≥100 mg/dL roughly doubles risk. In those with ASCVD and elevated Lp(a), adding a PCSK9 mAb with proven CV benefit when LDL‑C goals are not met is recommended (Class I).
Your role: in high‑yield cases (young MI, stroke, heavy family history), order Lp(a) during admission and hand off its interpretation to cardiology or lipid clinic with a note that elevated levels warrant more intensive LDL‑C lowering.
Risk tools and imaging: what do you need to know?
PREVENT equations (C‑P‑R model)
You may not be the one running risk calculators in the ED, but you will see PREVENT‑derived risk printed in discharge summaries. For adults 30–79 with LDL‑C 70–189 mg/dL and no ASCVD or subclinical disease, PREVENT‑ASCVD equations are now the preferred tool (Class I).
The guideline recommends a C‑P‑R framework:
Calculate PREVENT 10‑year (and 30‑year if 30–59 years).
Personalise with risk enhancers (e.g., Lp(a), ApoB, adverse pregnancy history, CKM syndrome, inflammatory disease).
Reclassify with Coronary Artery Calcification (CAC) if decisions remain uncertain in intermediate or select borderline risk patients.
For acute care physicians, the key is recognising that borderline risk is no longer “ignore” territory; it’s a zone where risk enhancers and CAC can tip you toward statins.
CAC and incidental findings
Coronary artery calcium is now a major decision tool:
In intermediate‑risk and selected borderline‑risk adults with no ASCVD, if you’re unsure about LLT, CAC should be used (Class I).
CAC thresholds tie directly to LDL‑C goals:
CAC 100–299 or ≥75th percentile: recommend LLT to LDL‑C <70 and non‑HDL‑C <100.
CAC 300–999: treat to at least LDL‑C <70, and it is reasonable to intensify toward <55 and non‑HDL‑C <85 (I/IIa).
CAC ≥1000: treat like very‑high‑risk ASCVD with LDL‑C <55 and non‑HDL‑C <85 (Class I).
Importantly, incidental CAC on non-cardiac CT (e.g., HRCT chest, CT aorta, CTKUB) “should be considered” in LLT decisions (Class I).
Your role: when you see “moderate‑severe coronary calcification” in a CT report on an ED or ward patient, don’t ignore it. Document that this is subclinical ASCVD and that aggressive LLT and risk factor modification are indicated.
Triglycerides, diet, and the RDN: practical bedside moves
The lifestyle section may seem “clinic‑heavy”, but there are ED/ward implications:
For TG ≥1000 mg/dL, involving an RDN is Class I; for TG 150–999 mg/dL with CKM features it is reasonable (IIa).
Core diet messages for acute care:
Eliminate alcohol in severe hyperTG and pancreatitis.
Restrict total fat in TG ≥1000 mg/dL, and reduce added sugars and refined carbs across hyperTG strata.
Encourage modest weight loss (5–10%) and progressive physical activity once stable.
You may not design the whole diet plan, but putting “RDN referral” and “alcohol elimination” into your initial orders is now guideline‑aligned.
New drugs: what you need to recognise by name
You will increasingly see these agents in medication histories and discharge plans:
PCSK9 mAbs (evolocumab, alirocumab)
Indicated for severe hypercholesterolemia and very‑high‑risk ASCVD not at LDL‑C goals despite maximally tolerated statin ± ezetimibe (Class I/IIa).
Bempedoic acid
Oral agent recommended or reasonable in severe hypercholesterolemia and ASCVD when LDL‑C remains above goal on statin ± ezetimibe or in statin‑intolerant cases (Class I/IIa).
Inclisiran
Twice‑yearly siRNA, reasonable in severe hypercholesterolemia or very‑high‑risk ASCVD when PCSK9 mAbs are not tolerated or available, or when less frequent dosing is preferred (IIa; outcomes pending).
Olezarsen
ApoC3 inhibitor recommended in familial chylomicronemia with TG ≥1000 mg/dL to reduce TG and pancreatitis (Class I).
Your role is not to initiate these from the ED in most settings, but to recognise their indications, avoid harmful drug interactions, and avoid inadvertently stopping them on admission unless absolutely necessary.
Where this guideline is strong, and where you should be cautious
Strengths for acute care:
Clear Class I mandates for high‑intensity statin use in all appropriate ASCVD admissions.
Explicit LDL‑C and non‑HDL‑C targets that make discharge planning goal‑oriented.
Structured handling of severe hyperTG and pancreatitis risk, including diet and new therapies.
Integration of Lp(a), ApoB, and CAC to explain “why did this young patient infarct?”
Cautions from the ED/ICU perspective:
Complexity: PREVENT, risk enhancers, ApoB, Lp(a), CAC, and multiple LDL targets are too much to carry in memory; local protocols and order sets will be crucial.
US‑centric risk: PREVENT is not calibrated for South Asians and may underestimate risk; for Indian patients, have a lower threshold to treat.
Resource constraints: routine Lp(a), ApoB, CAC and advanced drugs may not be widely available; you may need to adapt the principles (aggressive statin, early identification of FH) to what is feasible in your context.