
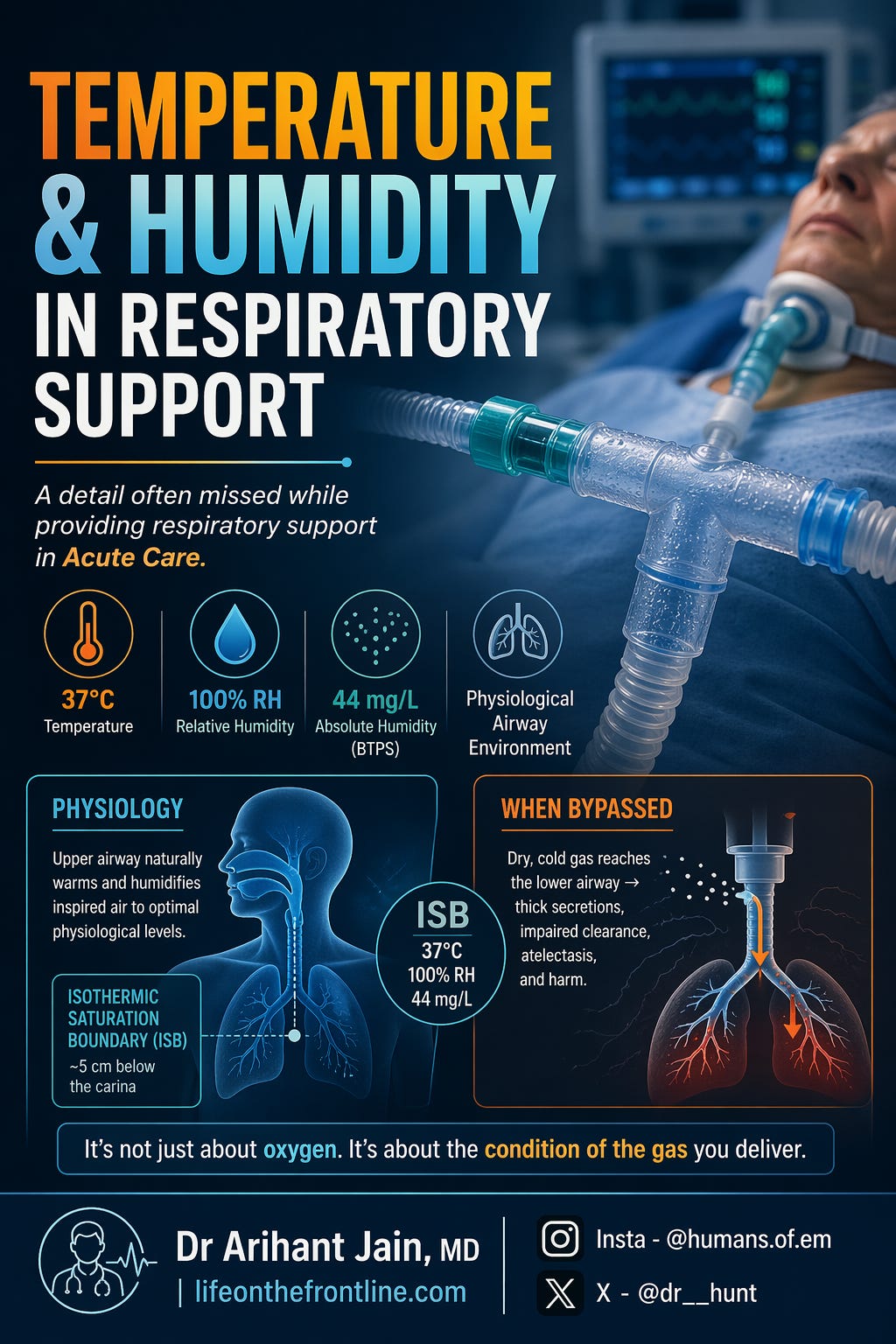
Temperature & Humidity in Respiratory Support
A detail often missed while providing respiratory support in Acute Care.

Case Scenario
A 58-year-old patient with a tracheostomy, in ED, is on:
High-flow oxygen via T-piece
Flow: 15 L/min
Over the next 12 hours, you notice:
Increasingly thick secretions
Frequent suctioning
Rising airway pressures
Intermittent desaturation
👉 The setup seems “adequate” — oxygen is being delivered.
👉 But is something fundamentally wrong?
❗ The Hidden Problem
Yes — this patient is receiving high-flow dry gas.
The upper airway has been bypassed (tracheostomy)
The natural system for:
Heating
Humidification
is completely lost
And now:
You are delivering high flow + dry oxygen directly into the trachea
👉 This is not just suboptimal — it is physiologically harmful
Why This Happens (Link to Physiology)
Under normal conditions:
Inspired air reaches 37°C, 100% RH, ~44 mg/L AH at the Isothermic Saturation Boundary (ISB)
Located ~5 cm below the carina (Al Ashry & Modrykamien, 2014)
But in this patient:
No nasal conditioning
No pharyngeal humidification
No heat exchange
➡️ ISB shifts distally
➡️ Lower airway forced to compensate (which it cannot adequately do)
Consequences You Are Seeing
Thick, inspissated secretions
Mucociliary dysfunction
Increased airway resistance
Risk of tube blockage
Atelectasis
(Re et al., 2024; Al Ashry & Modrykamien, 2014)
The Core Question
👉 Are you delivering oxygen… or are you delivering injury?
Transition to Concept
This scenario highlights a fundamental truth:
Oxygen therapy is not just about FiO₂ — it is about gas conditioning
To understand this, we need to revisit:
Absolute vs Relative Humidity
Temperature–humidity relationship
The Isothermic Saturation Boundary
…and how these principles dictate device selection across oxygen therapy, NIV, and ventilation
1. Fundamental Physiology
Absolute vs Relative Humidity
Absolute humidity (AH) is the mass of water vapor present in a given volume of gas (mg H₂O/L) and represents the true water delivered to the airway.
Relative humidity (RH) is the ratio of actual water content to the maximum possible at that temperature, expressed as a percentage.
A key physiological principle:
↑ Temperature → ↑ water-carrying capacity → ↓ RH
↓ Temperature → ↑ RH → → condensation beyond saturation
This explains condensation (“rainout”) in ventilator circuits, where cooling of saturated gas leads to water deposition (Re et al., 2024).
Isothermic Saturation Boundary (ISB)
The ISB is the point where inspired gas reaches:
37°C
100% RH
~44 mg/L AH (BTPS)
Normally located ~5 cm below the carina (Al Ashry & Modrykamien, 2014).
Clinical Relevance of ISB Shift
Bypassing upper airway (ETT, tracheostomy, high flows) → ISB shifts distally → lower airway exposed to dry gas →
Mucociliary dysfunction
Thick secretions
Increased airway resistance
Atelectasis
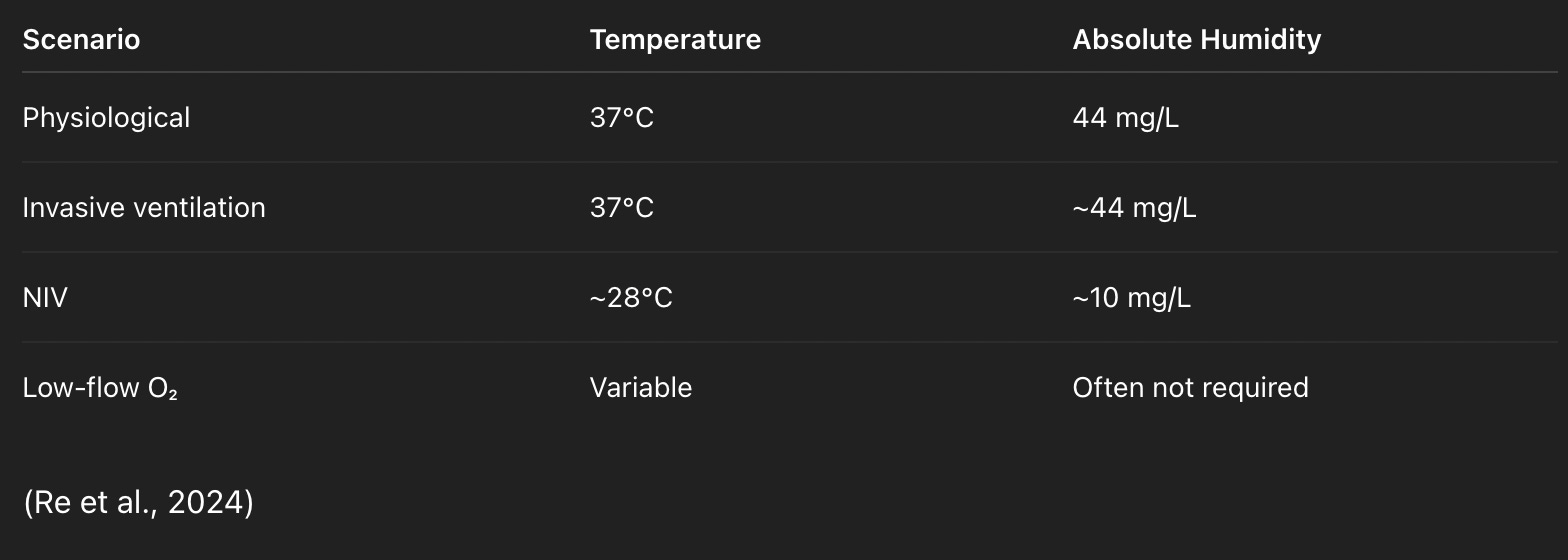
2. Translating Physiology → Targets
3. Device Selection Across Respiratory Support
A. Low-Flow Oxygen
Usually no humidification needed
Add if prolonged or >4–5 L/min
🔧 Bubble humidifier
Gas bubbled through water (low efficiency)
Limited AH delivery
(Concept illustrated in humidifier types, Al Ashry & Modrykamien, 2014)
B. High-Flow Nasal Oxygen (HFNC)
High flows overwhelm native humidification
🔧 Heated active humidifier (passover type)
Heated circuit prevents cooling
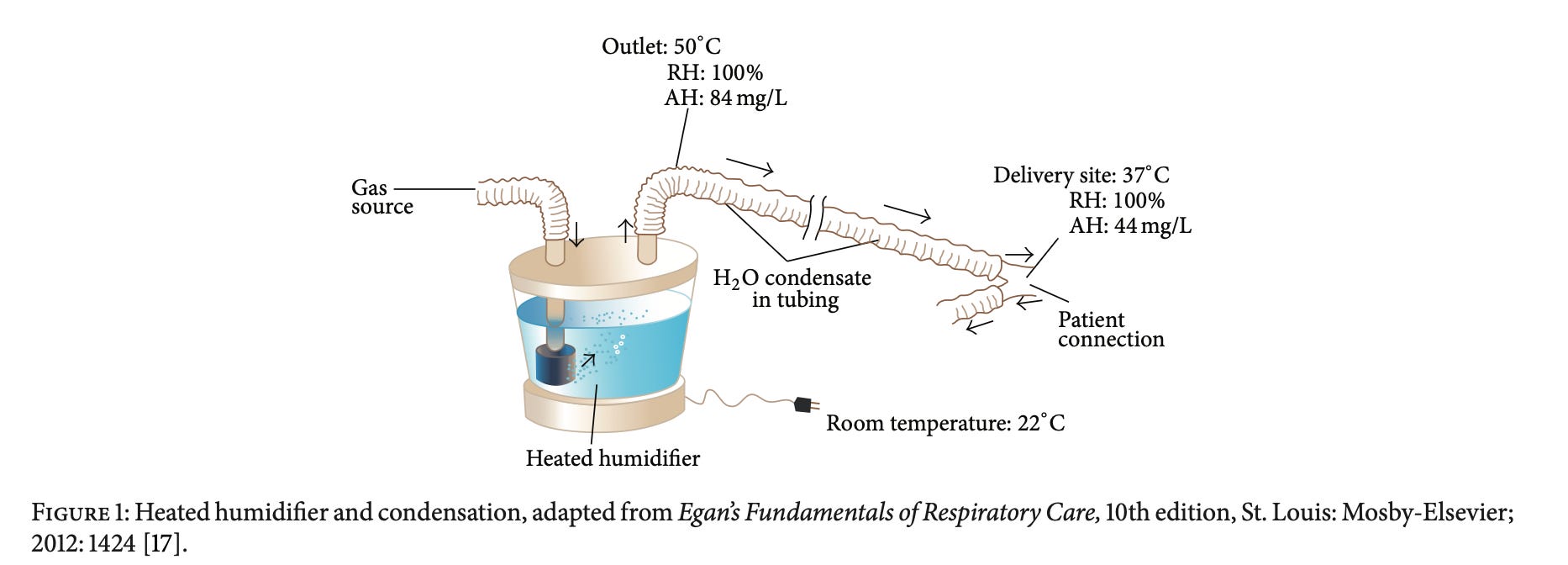
Based on Figure 1 concept (heated humidifier + condensation):
Gas leaves fully saturated
Cooling → condensation → reduced effective delivery
(Al Ashry & Modrykamien, 2014)
C. Non-Invasive Ventilation (NIV)
Target:
~28°C
~10 mg/L AH
(Re et al., 2024)
🔧 Device:
Prefer active humidifier
💡 Rationale:
Dry pressurized gas + high flow → overwhelms natural airway conditioning
D. Invasive Mechanical Ventilation
Mandatory humidification
Target:
37°C
44 mg/L AH
(Re et al., 2024)
Device Options
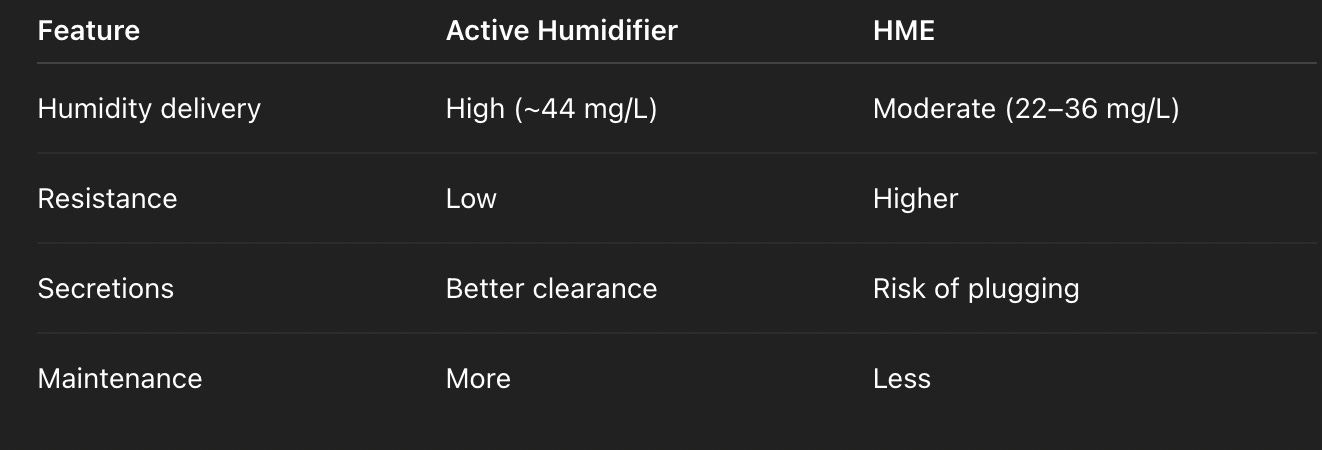
1. Active Humidifiers
Passover (most common) - learn modern concepts at Re et al., 2024
Bubble / counterflow variants
✔ High humidity delivery
✔ Ideal for thick secretions
⚠️ Issues:
Condensation
Circuit maintenance
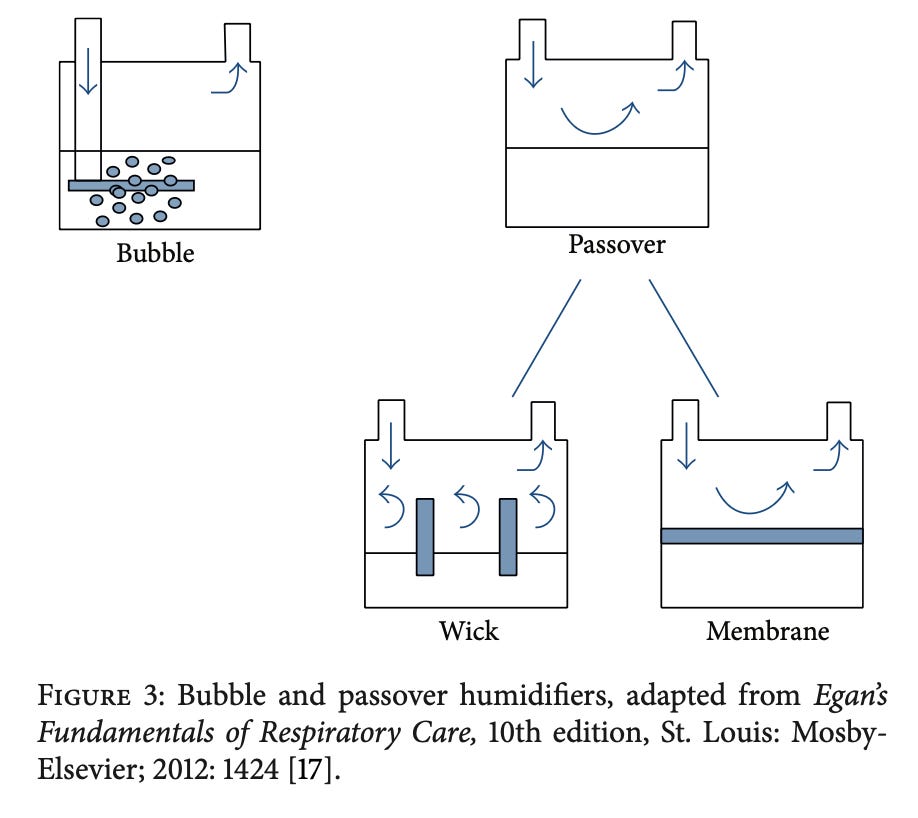
(Figure 3: humidifier types, Al Ashry & Modrykamien, 2014)
💧 2. Passive Humidifiers
(HME – Heat & Moisture Exchangers)
Placed between Y-piece and patient
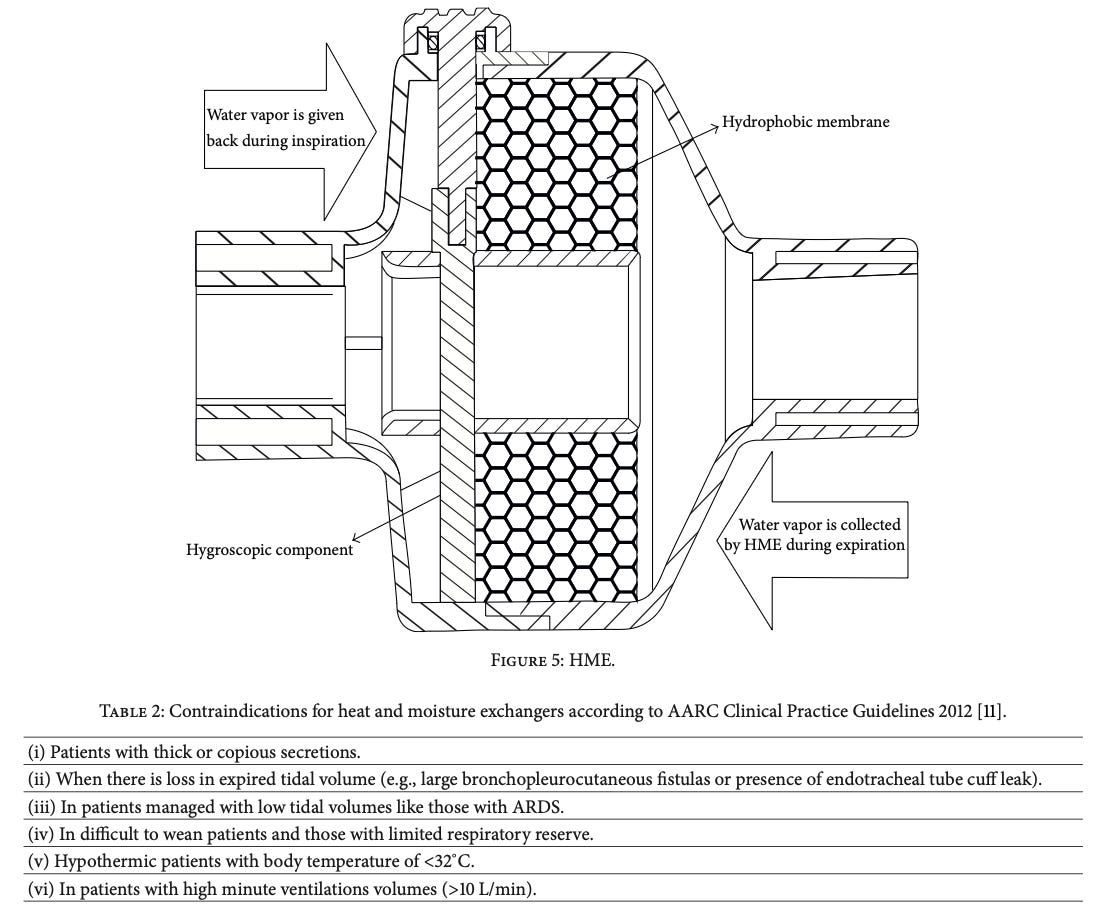
(Figure 5: HME function, Al Ashry & Modrykamien, 2014)
Types of Passive Humidifiers
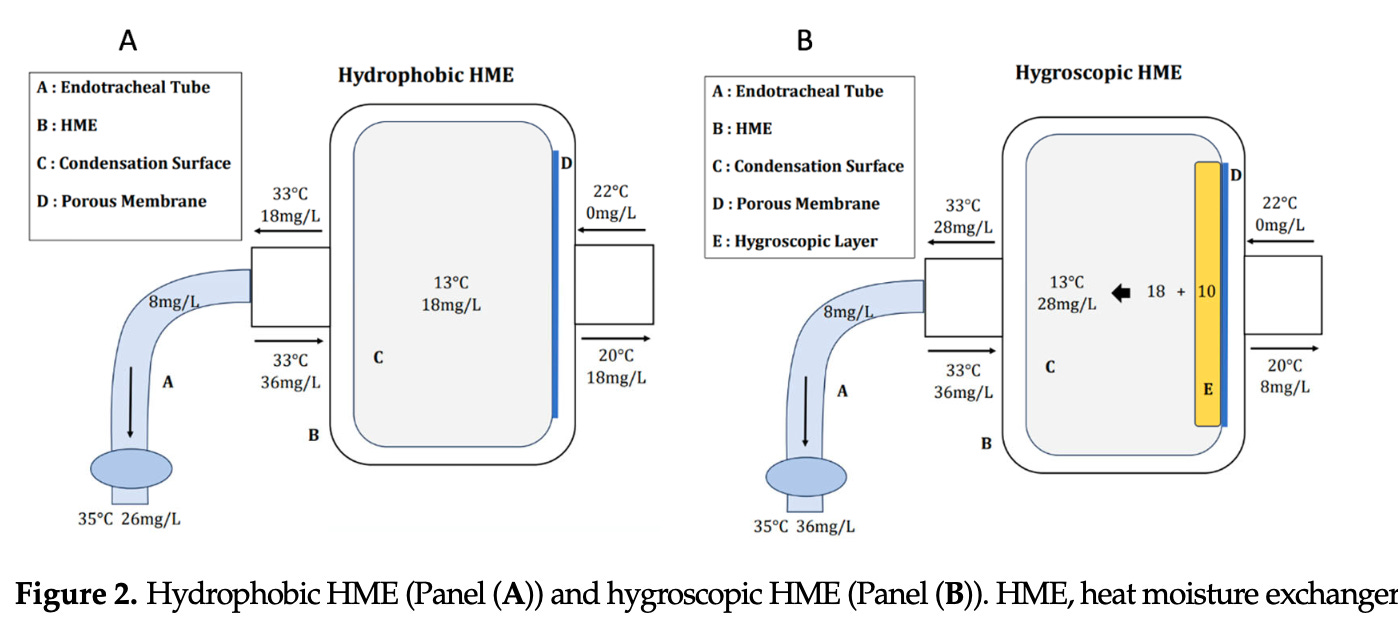
A. Hydrophobic HME
Structure:
Water-repellent membrane
Low thermal conductivity
Mechanism:
Condenses exhaled moisture on surface
Returns it during inspiration
Performance:
Lower humidity delivery (~22–28 mg/L)
Limitations:
Less efficient heat transfer
Greater risk of airway narrowing and secretion retention
👉 Clinically:
Less preferred in ICU practice
B. Hygroscopic HME
Structure:
Contains hygroscopic salts (e.g., calcium chloride, lithium chloride)
Mechanism:
Chemical attraction of water molecules
Stores more moisture than hydrophobic HMEs
Performance:
Higher AH (~28–36 mg/L)
Better approximation of physiological humidity
(Re et al., 2024; Al Ashry & Modrykamien, 2014)
C. Combined Hygroscopic + Hydrophobic (Modern HMEs)
Combine:
Hygroscopic element (moisture retention)
Hydrophobic filter (barrier + structure)
✔ Best balance:
Improved humidification
Infection control
D. HME with Filter (HMEF)
Adds bacterial/viral filtration
Types:
Pleated (mechanical) → better filtration, ↑ resistance
Electrostatic → lower resistance
Practical Comparison
🚫 Avoid HME in:
Thick secretions
ARDS (low tidal volume)
High minute ventilation
Hypothermia
(Al Ashry & Modrykamien, 2014)
E. Tracheostomy
Complete bypass of upper airway
🔧 Use:
Heated humidifier OR
Heated trach collar OR
Tracheostomy HME
Essential to prevent:
Crusting
Tube blockage
4. Clinical Pitfalls
Dry circuit ≠ adequate humidification
Condensation ≠ incorrect setup
Ignoring environment (temperature, flow) affects performance
(Al Ashry & Modrykamien, 2014)
📌 Follow for more
Dr Arihant Jain, MD
lifeonthefrontline.com
Instagram: @humans.of.em
X - dr__hunt
Final Framework
Airway bypassed? → Full humidification
High flow? → Active humidifier
Closing Insight
👉 Humidity is a physiological variable—not an accessory setting
It directly impacts:
Gas exchange
Airway resistance
Secretion clearance
Patient outcomes
References
Al Ashry HS, Modrykamien AM. Humidification during mechanical ventilation in the adult patient. 2014.
Re R, Lassola S, De Rosa S, Bellani G. Humidification during invasive and non-invasive ventilation: A starting tool kit for correct setting. 2024.