
Syncope: A Practical Approach That Won’t Miss the Killer Diagnoses
Syncope is one of those ED presentations that looks “simple”… right up until it isn’t.

A well-appearing patient walks in saying, “I fainted for a few seconds.” Vitals normal now. They’ve already recovered. The family wants to go home. And yet — somewhere in that syncope pile hides VT, complete heart block, PE, aortic catastrophe, GI bleed, and subarachnoid hemorrhage.
Your job is not to give a perfect diagnosis to every syncope patient.
Your job is to answer three questions:
Was this true syncope?
Is there a serious cause that can kill them soon?
Do they need monitoring/admission — or can they safely go home?
This post gives a structured approach — consistent with how Rosen’s teaches ED reasoning and how EM:RAP frames bedside decision-making — simple, high-yield, and disposition-focused.
Step 1: Confirm it is actually syncope
Syncope is not just “any collapse.”
True syncope is:
transient loss of consciousness
due to global cerebral hypoperfusion
rapid, spontaneous recovery
no persistent neurologic deficit afterward
(Sandhu & Sheldon, 2019)
The most common trap: calling everything syncope
Before you go into risk stratification mode, exclude the mimics:
Seizure clues
prolonged post-ictal confusion
tongue bite (especially lateral)
witnessed tonic–clonic activity
incontinence
(Sandhu & Sheldon, 2019)
Other TLOC mimics
hypoglycemia
intoxication
concussion
psychogenic pseudosyncope
(Sandhu & Sheldon, 2019)
If the story is not clearly syncope, don’t force it into the syncope pathway.
Step 2: Stabilize first, then stratify
Syncope is sometimes the symptom of shock or impending collapse.
So the opening move is not history. It’s this:
✅ ABC
✅ Monitor
✅ 12-lead ECG
✅ Bedside glucose
✅ IV access if ill-appearing / high risk
(Furlan et al., 2024)
Red flags requiring immediate resuscitation / urgent workup
hypotension or shock (SBP <90 or persistent abnormal vitals)
chest pain, dyspnea, hypoxia
persistent altered sensorium
focal neurologic deficit
major trauma from fall
GI bleed signs or severe anemia suspicion
(Furlan et al., 2024)
In these cases: stop talking and start treating.
Step 3: The “Big 4” ED workup (for every syncope patient)
This is the heart of the ED approach:
1) History (still the highest yield test)
Focus on 4 elements:
A. Circumstances
exertional? (danger)
supine? (danger)
after standing? (orthostatic)
during cough/micturition/defecation? (situational reflex)
(Hatoum & Sheldon, 2021)
B. Prodrome
nausea, warmth, diaphoresis, visual dimming → reflex/vasovagal pattern
sudden collapse with no warning → arrhythmia concern
(Hatoum & Sheldon, 2021)
C. Cardiac background
structural heart disease, CHF, CAD, arrhythmia history
pacemaker/ICD present
(Reed, 2018)
D. Medications
antihypertensives, diuretics
QT-prolonging meds
insulin/oral hypoglycemics
(Hatoum & Sheldon, 2021)
Also ask:
family history of sudden death
(Reed, 2018)
2) Examination
Full vitals + focused exam.
Orthostatics
Orthostatic BP/HR is not glamorous — but useful when done properly and interpreted in context.
(Sandhu & Sheldon, 2019)
Cardiac exam
Murmurs? Think aortic stenosis / HOCM risk with exertional syncope.
Neuro exam
Syncope should not cause focal deficits. If it does, you’re off the syncope pathway.
3) ECG — mandatory in every syncope
The ECG is the universal syncope test.
(Sandhu & Sheldon, 2019)
But don’t stare at it “generally.” Pattern-scan it for lethal diagnoses.
WOBBLER: ECG red flags in syncope
W — WPW / pre-excitation (delta wave, short PR)
O — Obstruction patterns (LVH strain; RV strain if PE context)
B — Brugada (coved ST elevation V1–V3)
B — Blocks / Brady (2nd/3rd degree AV block, bifascicular block + syncope, pauses)
L — Long QT / Short QT (QTc >480 ms is high risk)
E — Epsilon / cardiomyopathy patterns (ARVC clues: epsilon wave, T inversion V1–V3)
R — Regional ischemia / infarct (ST changes, new Q waves)
(Sandhu & Sheldon, 2019; Hatoum & Sheldon, 2021)
Take-home: The ECG in syncope is not to “support vasovagal.”
It is to catch sudden-death patterns fast.
Normal ECG ≠ safe, but abnormal ECG = higher risk until proven otherwise.
4) Focused tests only (avoid shotgun workup)
Don’t do reflex “syncope panels.”
Instead:
Labs only if indicated
Hb if bleeding suspected
electrolytes if vomiting/diuretics/QT concerns
creatinine if dehydration
β-hCG where appropriate
troponin only if ACS suspected / CSRS calculation in indeterminate cases
(Furlan et al., 2024)
Imaging only for a reason
CT head: focal deficit, head trauma, severe headache, anticoagulated fall
CTPA: only when PE suspected clinically
(Sandhu & Sheldon, 2019)
The ED “Deadly Syncope Six”
If you want a high-yield mnemonic list:
FAST + B
Fatal arrhythmia
Aortic catastrophe (dissection/AAA rupture)
Severe structural heart disease (AS/HOCM/tamponade)
Thromboembolism (massive PE)
Bleeding (GI bleed/ectopic)
If you’ve reasonably ruled these out → most syncope becomes safe disposition + follow up.
Step 4: Who actually needs risk stratification?
Risk stratification is NOT for every syncope patient
In the ED, most cases can be triaged into one of two buckets after history + vitals + ECG:
Group A: Cause identified / likely benign (no score needed)
These are patients with a high-likelihood diagnosis at the bedside:
classic vasovagal trigger + prodrome
clear orthostatic hypotension (dehydration/medication) with improvement after treatment
no high-risk history features
normal exam + normal ECG
👉 These patients don’t need syncope scores. Use the diagnosis, treat the cause, discharge with precautions.
(Reed, 2018; Sandhu & Sheldon, 2019)
Group B: High-risk red flags present (no score needed)
These are “admit/monitor until proven otherwise” patients:
structural heart disease / CHF
exertional syncope
syncope while supine
palpitations immediately before event
no prodrome / instantaneous collapse
persistent hypotension/tachycardia
WOBBLER-positive ECG
(Reed, 2018; Hatoum & Sheldon, 2021; Furlan et al., 2024)
👉 Risk scores should not override these.
They already need telemetry / inpatient workup.
Group C: Indeterminate cause after ED evaluation (this is where scores belong)
This is the real “syncope risk stratification population”:
✅ after ED history + exam + vitals + ECG
✅ no obvious benign diagnosis
✅ no clear high-risk red flag that mandates admission
✅ but you still feel uncertainty
This is the risk group where:
observation vs discharge is unclear
short-term serious event risk matters
expedited outpatient workup pathways matter
(Möckel et al., 2024; Wakai et al., 2024)
So: scores are meant for indeterminate syncope after initial ED evaluation
This is crucial:
Syncope risk scores should be used mainly when the cause remains indeterminate after initial ED evaluation, to guide disposition and follow-up.
They are not needed for an obvious vasovagal story, and they should never override high-risk red flags.
This aligns with ED evidence that decision tools are adjuncts, not replacements for bedside judgement.
(Wakai et al., 2024; Broek et al., 2023)
1) Canadian Syncope Risk Score (CSRS) — best ED tool
Most validated ED score predicting 30-day serious adverse events, and incorporates physician ED impression.
(Thiruganasambandamoorthy, 2016; Thiruganasambandamoorthy et al., 2020)
Predictive performance:
External validation AUC ≈ 0.91 (high discrimination)
(Thiruganasambandamoorthy et al., 2020)
Risk categories in validation:
very low risk ~0.2% serious outcome
low risk ~0.7%
very high risk up to ~51%
(Thiruganasambandamoorthy et al., 2020)
ED framing:
CSRS is a good “permission tool” to discharge when uncertain — but only after you’ve excluded high-risk red flags.
2) San Francisco Syncope Rule (SFSR) — fast but less reliable
Still taught because it’s simple, but meta-analyses show performance is moderate and inconsistent across settings.
Meta-analysis performance:
Sensitivity ≈ 86–87%
Specificity ≈ 48–49%
(Serrano et al., 2010; Saccilotto et al., 2011)
Meaning in practice:
tends to over-admit (low specificity)
not strong enough alone for safe discharge decisions
Mnemonic: CHESS (CHF, Hct <30, ECG abnormal, SOB, SBP <90)
3) ROSE rule — better specificity, but less practical
ROSE had:
Sensitivity 87.2%
Specificity 65.5%
NPV 98.5%
(Reed et al., 2010)
But it relies on labs such as BNP and FOBT, making it less ED-efficient in many systems.
Mnemonic: BRACES
(BNP, Bradycardia, Rectal blood, Anemia, Chest pain, ECG Q waves, SpO₂ ≤94%)
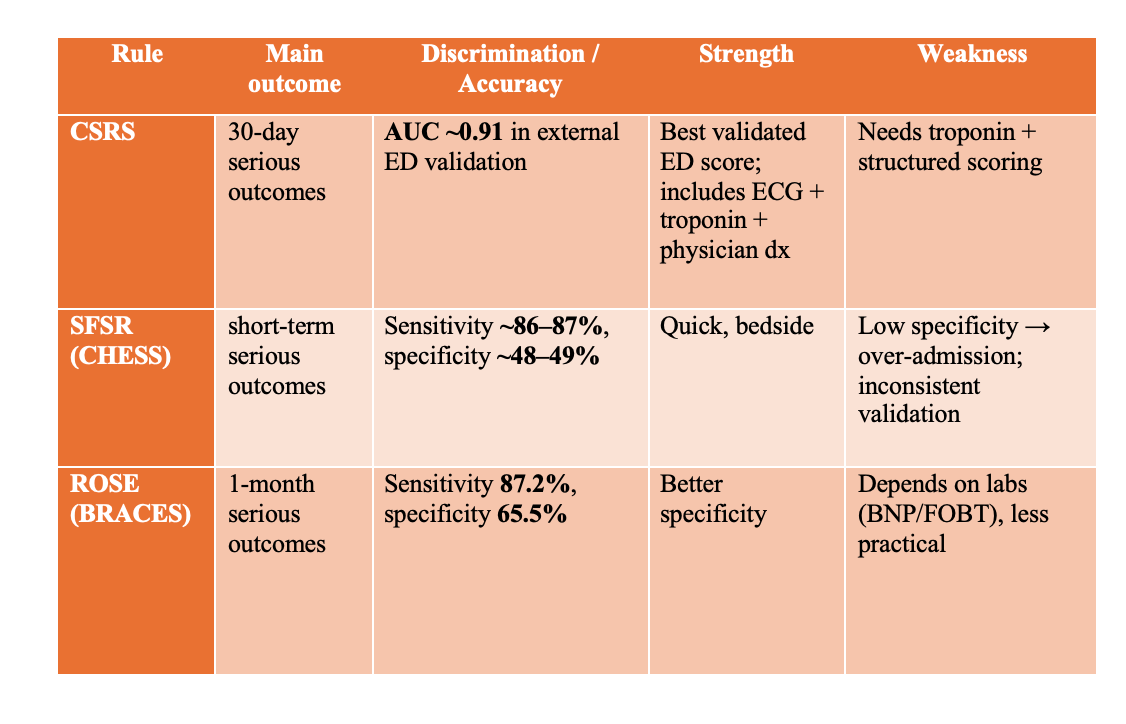
So:
CSRS wins overall discrimination (AUC)
SFSR is sensitive but nonspecific (safe-ish but admits too many)
ROSE improves specificity but is heavier on labs
Step 5: Who can be discharged?
Syncope Discharge Criteria (ED Checklist)
Discharge is reasonable when the patient is “Low-risk syncope” after ED evaluation.
The ED goal is not to label every cause — it’s to safely exclude serious disease.
✅ 1) Patient is stable in ED
Vitals normal after observation/treatment
No persistent hypotension
No persistent tachycardia
No hypoxia
Back to baseline mental status
No ongoing concerning symptoms
chest pain, dyspnea, severe headache, persistent neuro symptoms
✅ 2) Benign mechanism is likely
Any one of the following patterns fits:
A. Reflex / Vasovagal
typical trigger (pain/emotion/heat/prolonged standing)
prodrome (nausea, diaphoresis, warmth, visual dimming)
gradual onset + rapid recovery
B. Situational syncope
micturition / defecation / cough / swallow
C. Orthostatic syncope
postural trigger (standing up)
dehydration/medication-related
improves after fluids or med adjustment
If the cause remains indeterminate, move to intermediate-risk pathway (risk score/observation).
✅ 3) No high-risk history features
All must be absent:
no known structural heart disease / CHF
no syncope during exertion
no syncope while supine
no palpitations just before syncope
no family history of sudden cardiac death
no recurrent unexplained syncope with injury
✅ 4) ECG is reassuring (WOBBLER negative)
No:
AV block / pauses / severe bradyarrhythmia
ventricular arrhythmia
Brugada pattern
WPW / pre-excitation
long QT (esp QTc >480 ms)
ischemic changes
significant conduction disease (e.g., bifascicular block + syncope)
✅ 5) No dangerous alternative diagnosis suspected
No clinical concern for:
GI bleed / severe anemia
PE (dyspnea, hypoxia, pleuritic pain)
aortic dissection/AAA rupture
ectopic pregnancy (if applicable)
SAH/stroke (headache, neuro deficit)
major trauma requiring admission
✅ 6) Discharge is safe logistically
reliable supervision/support at home
clear follow-up plan (PCP/cardiology)
return precautions understood
advice on driving/work safety where appropriate
✅ “Grey-zone” discharge (when cause indeterminate)
If the cause is unclear but the patient remains stable and ECG is normal:
Use a syncope risk score (prefer CSRS)
Very low/Low risk → discharge + expedited follow-up
Medium → observation
High → admit/telemetry

References
Furlan L, Esposito G, Gianni F, Solbiati M, Mancusi C, Costantino G. Syncope in the Emergency Department: A Practical Approach. J Clin Med. 2024;13:3231. doi:10.3390/jcm13113231.
Reed MJ. Approach to syncope in the emergency department. Emerg Med J. 2019;36:108-116. doi:10.1136/emermed-2018-207767.
Allen R, deSouza I, Wakai A, Richards R, Ardilouze A, Dunne E, Rovic I, Benabbas R, Zehtabchi S, Sinert R. Hospitalize or discharge the emergency department patient with syncope? A systematic review and meta-analysis of direct evidence for SAEM GRACE. Acad Emerg Med. 2025. doi:10.1111/acem.15111.
Shen WK, Decker WW, Smars PA, Goyal DG, Walker AE, Hodge DO, Trusty JM, Brekke KM, Jahangir A, Brady PA, Munger TM, Gersh BJ, Hammill SC, Frye RL. Syncope Evaluation in the Emergency Department Study (SEEDS): A multidisciplinary approach to syncope management. Circulation. 2004;110:3636-3645. doi:10.1161/01.CIR.0000149236.92822.07.
Broek L, Ort B, Vermeulen H, Pelgrim T, Vloet L, Berben S. Risk stratification tools for patients with syncope in emergency medical services and emergency departments: a scoping review. Scand J Trauma Resusc Emerg Med. 2023;31:1-14. doi:10.1186/s13049-023-01102-z.
Hussein M, Cuncannon A. Syncope in the Emergency Department: A Guide for Clinicians. J Emerg Nurs. 2020. doi:10.1016/j.jen.2020.11.002.
Çanakçı M, Sevik O, Acar N. How Should We Approach Syncope in the Emergency Department? Current Perspectives. Open Access Emerg Med. 2022;14:299-309. doi:10.2147/OAEM.S247023.
Probst MA, Lin MP, Sze JJ, Hess EP, Breslin M, Frosch DL, Sun BC, Langan M, Thiruganasambandamoorthy V, Richardson LD. Shared Decision Making for Syncope in the Emergency Department: A Randomized Controlled Feasibility Trial. Acad Emerg Med. 2020;27:853-865. doi:10.1111/acem.13955.
Wakai A, Sinert R, Zehtabchi S, de Souza I, Benabbas R, Allen R, Dunne E, Richards R, Ardilouze A, Rovic I. Risk-stratification tools for emergency department patients with syncope: A systematic review and meta-analysis of direct evidence for SAEM GRACE. Acad Emerg Med. 2024;32:72-86. doi:10.1111/acem.15041.
Van Wijnen VK, Gans ROB, Wieling W, Ter Maaten JC, Harms MP. Diagnostic accuracy of evaluation of suspected syncope in the emergency department: usual practice vs ESC guidelines. BMC Emerg Med. 2020;20:1-10. doi:10.1186/s12873-020-00344-9.
Sandhu RK, Sheldon RS. Syncope in the Emergency Department. Front Cardiovasc Med. 2019;6:180. doi:10.3389/fcvm.2019.00180.
Möckel M, Janssens K, Pudasaini S, Riesgo L, Torrecilla F, Golea A, Reed M, Karamercan M, Cejas J, Laribi S. The syncope core management process in the emergency department: a consensus statement of the EUSEM syncope group. Eur J Emerg Med. 2024;31:250-259. doi:10.1097/MEJ.0000000000001146.
Hatoum T, Sheldon R. A Rational Evaluation of the Syncope Patient: Optimizing the Emergency Department Visit. Medicina (Kaunas). 2021;57:514. doi:10.3390/medicina57060514.
Syncope—definition, mimics, and emergency department evaluation. PubMed Central (PMC). PMCID: PMC6901601.
Syncope risk and safe discharge features (low-risk syncope). PubMed Central (PMC). PMCID: PMC5052859.
Intermediate-risk syncope and ED pathways/observation strategies. PubMed Central (PMC). PMCID: PMC11198953.
This is excellent ED cognition, distilled. I love how you anchor the entire encounter to the three questions that actually matter clinically: (1) true syncope vs mimic, (2) near-term lethal etiologies, (3) safe disposition, instead of letting the workup balloon into “syncope labs + CT head reflex“.
A few things that really stand out as high-yield and practice-changing:
1. Your “don’t force it into the syncope pathway” warning is gold. The biggest diagnostic errors I see are upstream: seizure/psychogenic TLOC/hypoglycemia masquerading as “syncope“.
2. The ECG pattern-scan mindset (WOBBLER) is exactly the right mental model. ECG is there to catch sudden-death patterns quickly. 
3. The Deadly Six / FAST + B framing is a perfect “don’t-miss” checklist that preserves bandwidth when the department is chaotic. 
4. And the nuance about who risk scores are actually for (indeterminate after H&P + vitals + ECG, never to override red flags) is the kind of teaching point that prevents both missed catastrophes and unnecessary admissions. 
If more syncope evaluations looked like this (structured, disposition-focused, and physiologically honest) we’d have fewer missed killers and a lot less iatrogenic testing.
Thanks! so organized 👌 😍 🙌