
Sepsis in 2026: Smarter, Earlier, Individualized
A practical framework for acute care clinicians navigating shock, organ failure, and stewardship at the bedside.

Sepsis Is Not a Bundle. It’s a Physiology Problem.
Sepsis management in emergency and acute care does not fail because we lack guidelines.
It fails when we mistake protocol compliance for physiologic care.
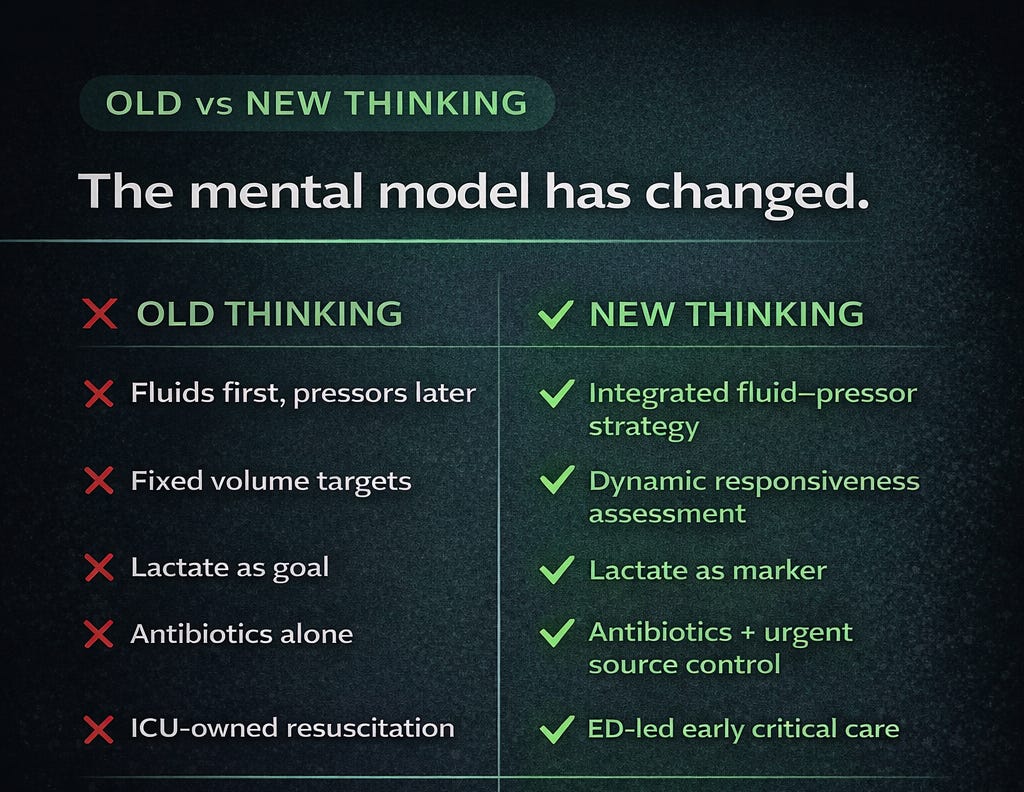
Across emergency departments, wards, and ICUs, the modern understanding of sepsis is evolving. The shift is subtle but profound:
From rigid bundles → to individualized, physiology-guided resuscitation.
For acute care clinicians, this is not an academic nuance. It is the difference between fluid overload and organ recovery. Between delayed vasopressors and preserved perfusion. Between antibiotics alone and definitive source control.
Let’s break this down pragmatically.
1️⃣ Sepsis Is a Time-Critical Emergency — Like STEMI or Stroke
We would never wait for ST elevation to “fully declare itself” before activating a cath lab.
We should not wait for hypotension before activating a sepsis response.
Early recognition hinges on identifying:
Suspected infection plus
Evidence of organ dysfunction
Not just shock.
Red flags at the front door:
Altered mentation
Tachypnea
Rising oxygen requirement
Oliguria
Cool or mottled extremities
Elevated lactate despite preserved BP
The dangerous patient is often the one with “normal blood pressure.”
This is cryptic shock — where hypoperfusion precedes hypotension.
Acute care clinicians must integrate early warning scores with clinical gestalt. No scoring system replaces bedside judgment.
2️⃣ The First Hours Matter — But Not All Fluids Are Beneficial
The traditional 30 mL/kg reflex has simplified thinking — but oversimplification carries harm.
Excess fluid leads to:
Pulmonary edema
Delayed extubation
Worsened renal outcomes
Increased mortality in some subgroups
The emerging model is dynamic:
Small bolus (250–500 mL) → reassess → repeat if responsive
Use physiology to guide you:
Passive leg raise
Stroke volume change
Bedside echo (LV function)
Capillary refill
Urine output
Lactate trend (not single value)
Sepsis resuscitation should be a loop:
Resuscitate → Reassess → Redirect.
Not a one-time fluid event.
Particularly in elderly patients or those with heart failure, CKD, or cirrhosis, restraint is not undertreatment — it is precision.
3️⃣ Earlier Vasopressors Prevent Fluid Creep
Waiting to “finish fluids” before starting vasopressors is increasingly indefensible.
When hypotension persists after limited fluid resuscitation:
Start norepinephrine early.
Peripheral initiation via a well-functioning IV is acceptable.
Target MAP ≈ 65 mmHg, individualized to perfusion markers.
Earlier vasopressors:
Restore perfusion sooner
Limit excess fluid accumulation
Shorten time to hemodynamic stability
Septic shock is distributive at its core. Fluids alone cannot correct vasoplegia.
4️⃣ Antibiotics Are Urgent — But Source Control Is Definitive
Timely antibiotics save lives — especially in septic shock.
Early intravenous antibiotics remain the only intervention consistently associated with reduced mortality in sepsis — particularly in septic shock.
In patients with septic shock or life-threatening instability, antibiotics should be administered within 1 hour of recognition, after obtaining appropriate cultures if this does not cause delay.
In patients without shock, where diagnostic uncertainty exists, a short period of focused evaluation is reasonable. Current guidance supports administration within 3 hours if concern for infection persists, with closer monitoring throughout. The mortality signal for delay is strongest in shock; in stable patients, modest delays to improve diagnostic precision are unlikely to worsen outcomes.
Empirical therapy should reflect local resistance patterns and individual risk factors for drug-resistant organisms. Once microbiology data become available, prompt de-escalation to narrow-spectrum therapy is essential to limit antimicrobial resistance and toxicity.
Shorter courses (generally 5–7 days) are adequate for most infections unless there is deep-seated or complicated disease. Importantly, antibiotics are not definitive therapy when source control is required.
Modern sepsis care demands both urgency and stewardship —
1 hour for the unstable, 3 hours with thoughtful precision for the uncertain.
But antibiotics are not the endpoint. They are the bridge.
Definitive therapy often requires :- Source Control
Drainage
Debridement
Decompression
Device removal
Obstructed urosepsis.
Perforated viscus.
Necrotizing soft tissue infection.
Infected lines.
The emergency department must initiate source control conversations immediately — not defer them.
Time-to-source-control may matter as much as time-to-antibiotics.
5️⃣ Point-of-Care Ultrasound Is Now Foundational
Sepsis is hemodynamically heterogeneous.
Some patients are:
Pure vasoplegia
Septic cardiomyopathy
Mixed shock
Fluid responsive
Fluid intolerant
Without ultrasound, we are often guessing.
POCUS allows rapid differentiation:
LV systolic function
RV strain
IVC variability
B-lines (early pulmonary edema)
Pericardial effusion
Intra-abdominal source clues
Modern sepsis care in acute settings is incomplete without bedside echocardiographic assessment.
6️⃣ Organ Support Begins in the ED — Not in the ICU
Many decisive interventions occur before ICU transfer:
High-flow nasal oxygen
Noninvasive ventilation
Early intubation with hemodynamic preparation
Lung-protective ventilation
Vasopressor titration
Renal function surveillance
Disposition is not administrative. It is physiological triage.
Patients on vasopressors, escalating oxygen support, rising lactate, or evolving multi-organ dysfunction require ICU-level care — early.
Clear handovers must include:
Fluids administered
Current vasopressor dose
Lactate trajectory
POCUS findings
Source control plan
7️⃣ Stewardship and Individualization Matter
Sepsis pathways must balance urgency with precision.
Over-resuscitation harms.
Indiscriminate broad-spectrum antibiotics drive resistance.
Delayed de-escalation perpetuates ICU burden.
Clinical decisions must incorporate:
Age
Co-morbidities
Functional baseline
Patient preferences
Resource realities
Early goals-of-care discussions are not therapeutic defeat — they are ethical medicine.
The Shift We Must Embrace
The evolution in sepsis management is not about abandoning bundles.
It is about maturing beyond them.
Sepsis is not a protocol problem.
It is a physiology problem.
And physiology demands continuous reassessment.
Reference -
Singer M, Angus DC, Annane D, et al. Sepsis. Lancet. Published online February 26, 2026. doi:10.1016/S0140-6736(25)02422-5