
Resuscitation in Toxicologic Emergencies: How is it different?
Understanding how monitoring, ABCDE priorities, and cardiac arrest care change when the cause is a reversible toxin.

In the emergency department, poisoned patients initially appear similar to other critically ill patients: airway compromise, respiratory failure, hypotension, or altered mental status. Accordingly, the initial approach still follows the standard ABCDE framework and ACLS/BLS principles (Hüser et al., 2025; Lavonas et al., 2023).
However, once resuscitation begins, the philosophy of care diverges.
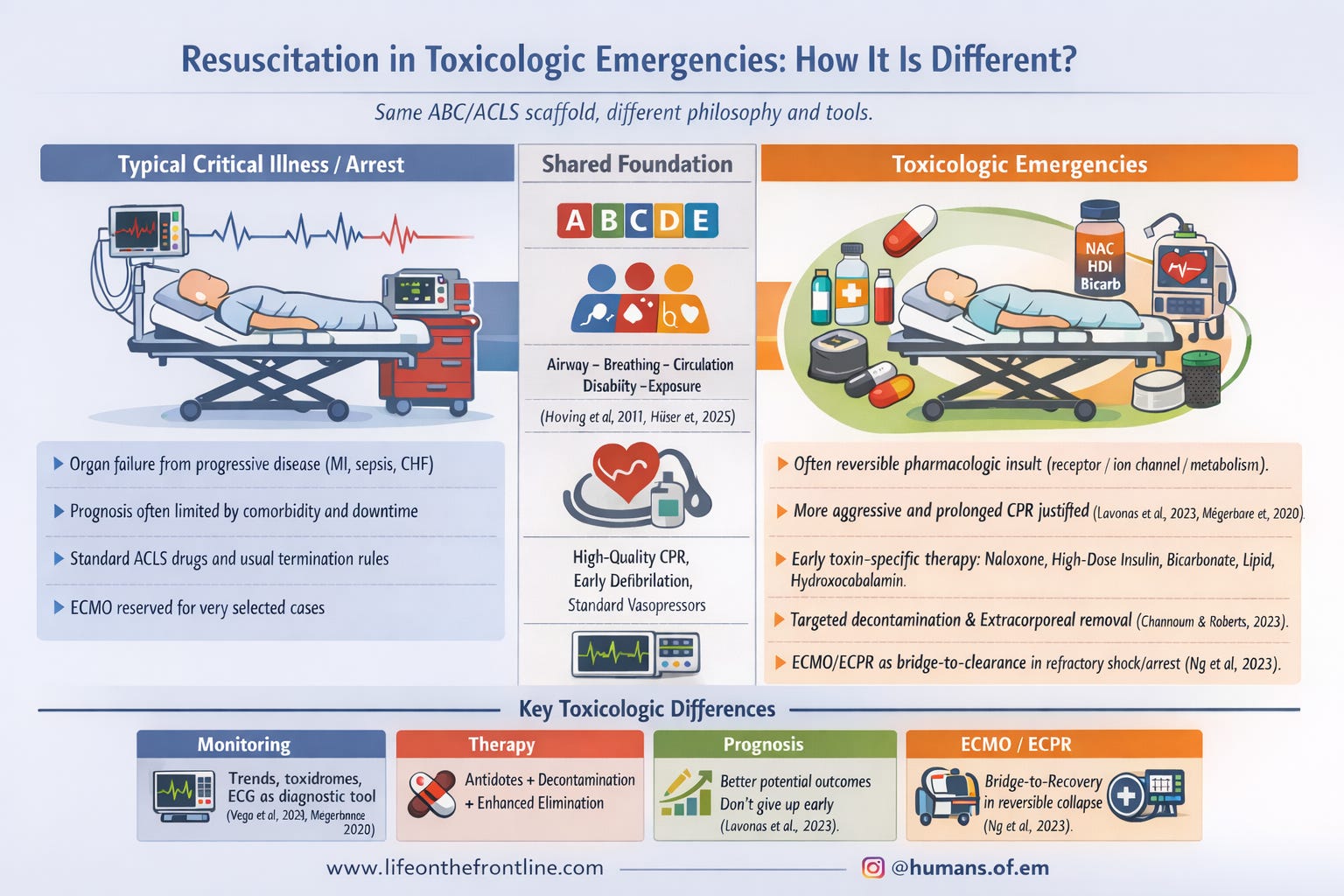
Unlike many medical emergencies where organ failure results from progressive disease processes (e.g., myocardial infarction, sepsis), poisoning frequently represents a potentially reversible physiologic disturbance caused by a toxin interacting with receptors, ion channels, or metabolic pathways (Mégarbane et al., 2020).
If the toxin can be neutralised, eliminated, or outlasted with supportive care, full recovery may occur even after severe shock or prolonged cardiac arrest (Lavonas et al., 2023).
This fundamental difference alters how clinicians monitor, resuscitate, and determine prognosis in poisoned patients.
Conceptual Differences in Toxicologic Resuscitation
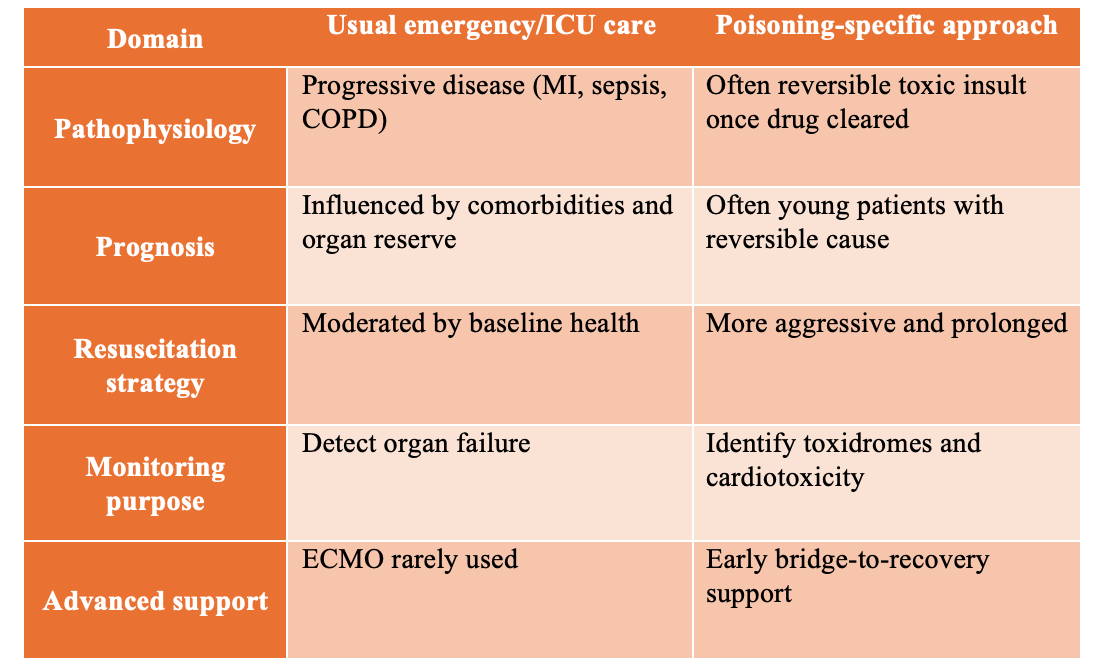
Poisoning therefore requires a different cognitive model:
Resuscitate aggressively because the underlying physiology may still be reversible (Lavonas et al., 2023; Mégarbane et al., 2020).
Monitoring Poisoned Patients: What Is Different?
Monitoring in toxicology is not purely supportive—it is diagnostic, prognostic, and therapeutic.
Clinical deterioration may occur abruptly due to delayed absorption, redistribution, or toxic metabolite formation. Therefore, continuous bedside observation and trend monitoring are essential (Vega et al., 2024; Hüser et al., 2025).
Standard parameters remain central:
Heart rate
Blood pressure
Respiratory rate
Oxygen saturation
Temperature
Level of consciousness (GCS)
However, clinicians focus heavily on trajectory rather than isolated measurements.
For example:
Gradual bradycardia and hypotension may suggest β-blocker or calcium channel blocker toxicity.
Increasing respiratory rate with metabolic acidosis may indicate salicylate poisoning.
Progressive sedation may signal opioid or sedative ingestion.
These patterns emerge because toxicodynamics evolve with time through delayed absorption, redistribution, or metabolite toxicity (Mégarbane et al., 2020).
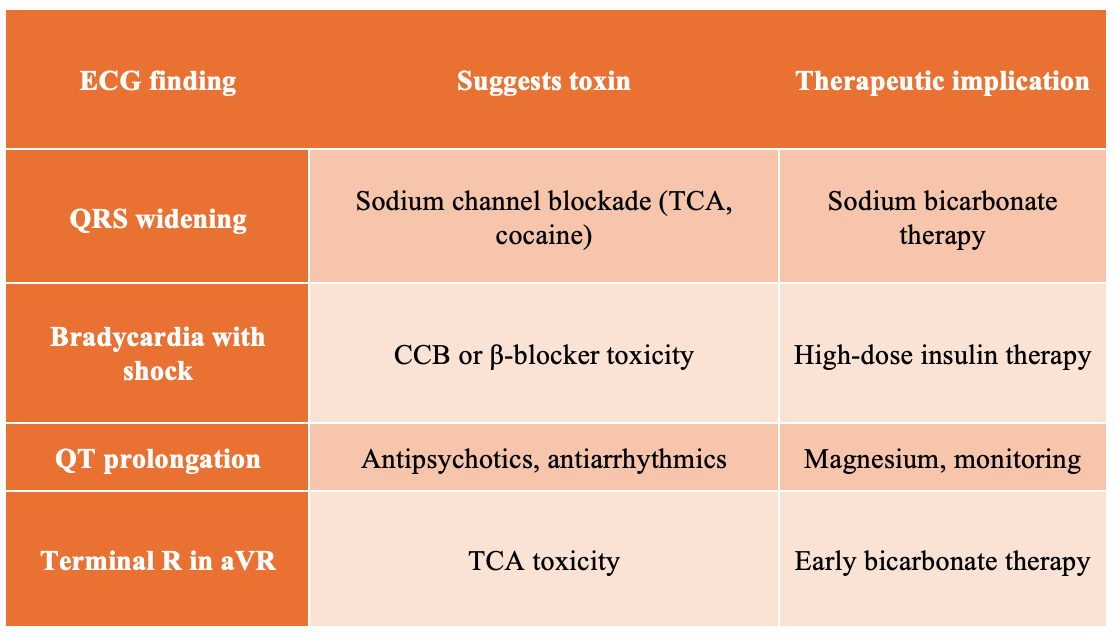
ECG Monitoring: The Toxicology Stethoscope
In poisoning, the ECG is both a monitoring tool and a diagnostic instrument.
Certain electrocardiographic findings strongly suggest specific toxin classes (Mégarbane et al., 2020).
Continuous telemetry is particularly important for exposures involving cardiotoxic drugs such as:
Tricyclic antidepressants
Antiarrhythmics
Antipsychotics
Cocaine
Calcium channel blockers
β-blockers (Mégarbane et al., 2020).
ECG abnormalities often precede hemodynamic deterioration, allowing earlier intervention.
Laboratory Monitoring: Targeted Rather Than Indiscriminate
Routine critical care investigations remain important:
Arterial or venous blood gases
Electrolytes
Creatinine
Glucose
Lactate
However, interpretation focuses on toxicologic patterns.
Examples include:
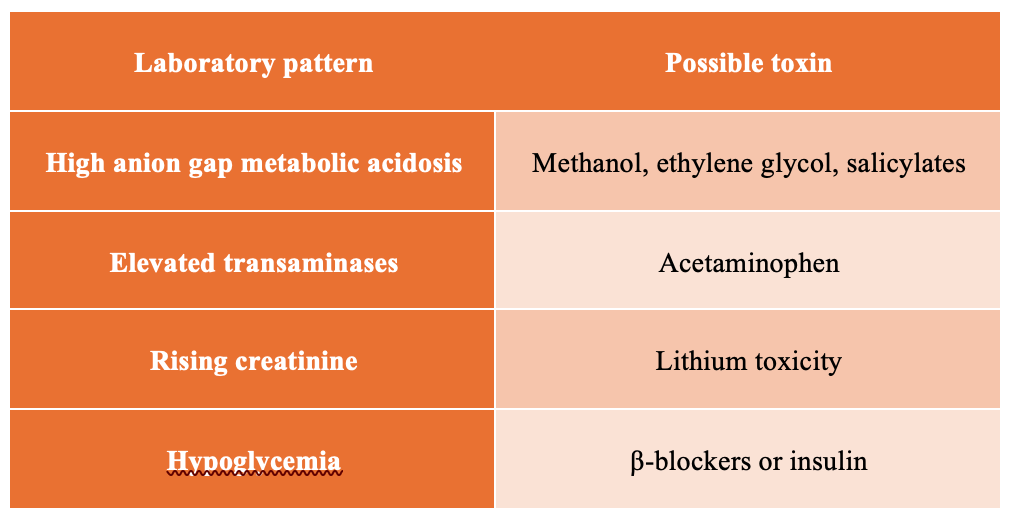
Toxin-specific laboratory assays are ordered only when they influence management, such as:
Acetaminophen levels
Salicylate levels
Lithium levels
Toxic alcohol levels (Bechtel & Holstege, 2022).
Routine broad toxicology screens rarely change acute management.
ABCDE in Poisoning: Same Structure, Different Thresholds
Although the ABCDE framework remains identical, poisoning alters the thresholds and priorities within each step (Hoving et al., 2011; Hüser et al., 2025).
Airway
Airway protection is often required earlier due to:
Rapid deterioration in consciousness
Recurrent seizures
High aspiration risk
Intubation is frequently indicated in:
Sedative overdose
Severe opioid intoxication
Massive ingestion with expected deterioration (Parris & Calello, 2022).
Breathing
Standard oxygen and ventilation strategies are combined with toxin-specific reversal therapies.
Examples include:
Naloxone for opioid-induced respiratory depression
Bronchodilators for inhalational exposures
Atropine and pralidoxime for organophosphate poisoning (Mégarbane et al., 2020).
Circulation
Circulatory failure in poisoning often requires toxin-directed therapy early in resuscitation.
Examples include:
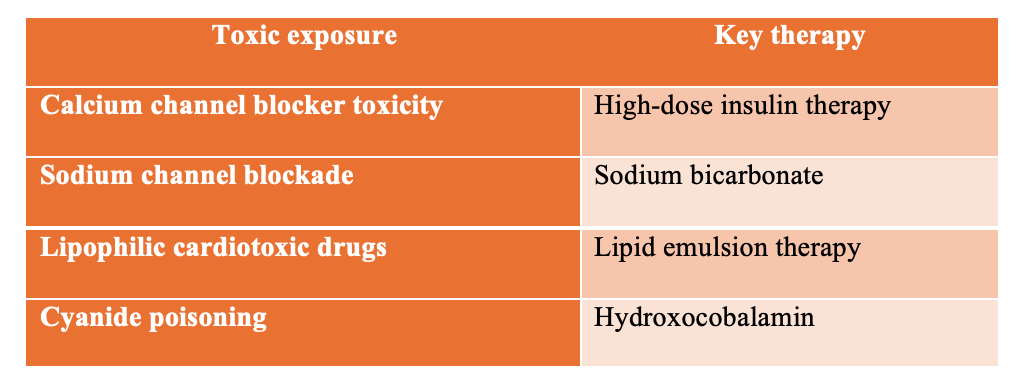
These interventions are frequently initiated before diagnostic confirmation because delay may worsen outcomes (Lavonas et al., 2023).
Disability
Neurologic assessment using GCS, pupillary examination, and glucose measurement guides antidote therapy and toxidrome recognition (Hoving et al., 2011).
For example:
Pinpoint pupils → possible opioid toxicity → naloxone trial
Seizures → benzodiazepine therapy
Anticholinergic syndrome → targeted management
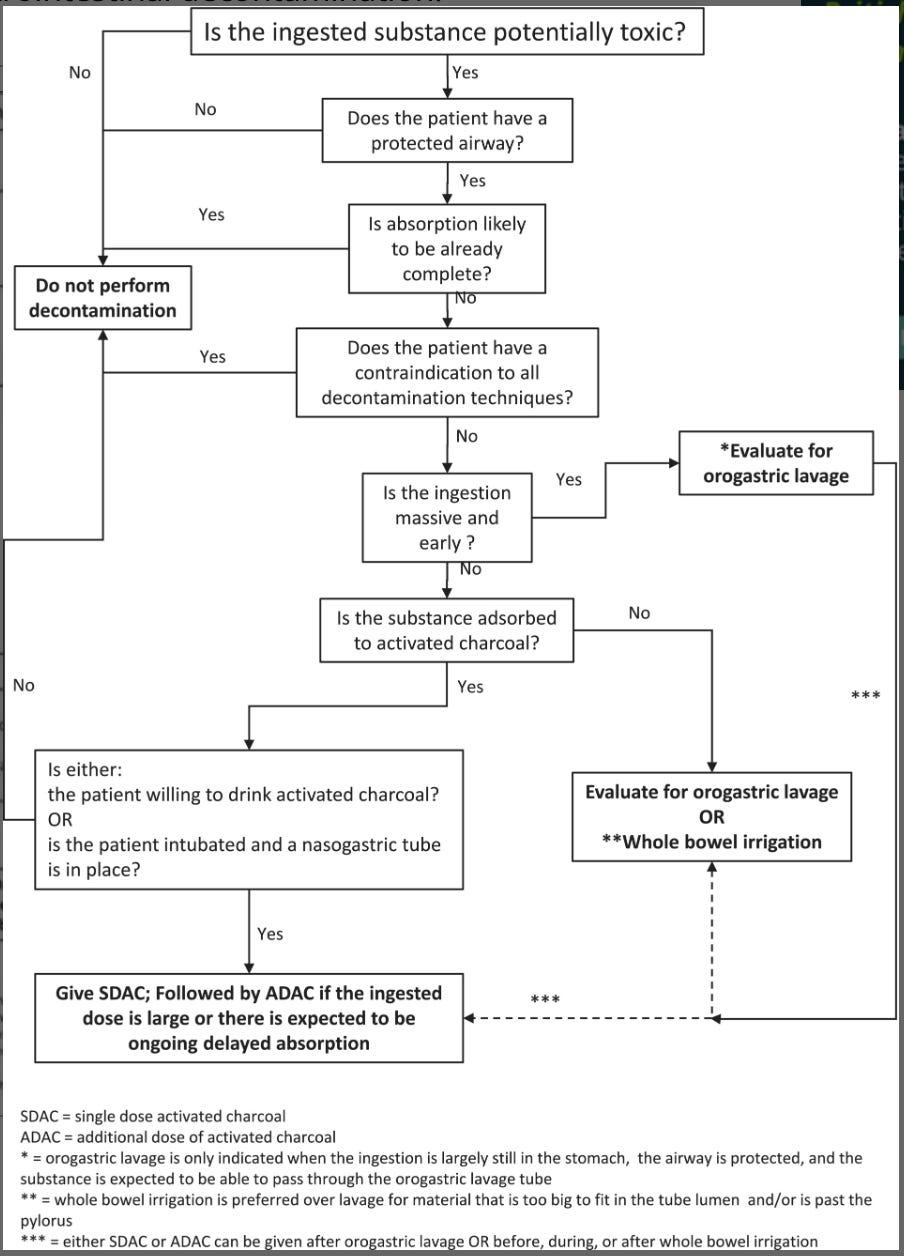
Detoxification: Unique to Toxicology
Unlike most critical illness, poisoning may require active toxin removal.
Gastrointestinal decontamination
Selective use of:
Activated charcoal
Whole bowel irrigation
Gastric lavage
Decision-making depends on:
Time since ingestion
Drug characteristics
Airway protection (Hüser et al., 2025).
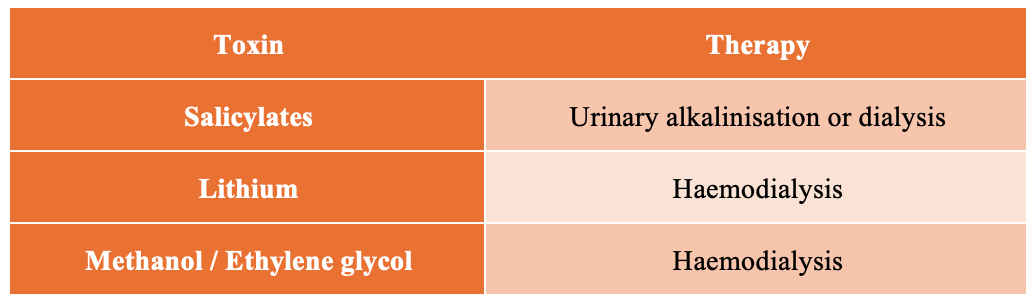
Enhanced elimination
Certain toxins can be removed through extracorporeal techniques.
Serial laboratory monitoring determines initiation and termination of therapy (Ghannoum & Roberts, 2023).
Cardiac Arrest in Poisoning: Why It Is Different
Toxicologic cardiac arrest differs from typical cardiac arrest in several important ways.
Many patients are:
Younger
Previously healthy
Experiencing reversible pharmacologic toxicity
Therefore prognosis may be better than in non-toxic cardiac arrest (Lavonas et al., 2023).
Longer and More Aggressive Resuscitation
Termination rules used in standard cardiac arrest may not apply in poisoning.
Resuscitation often involves:
Prolonged CPR
Early antidote administration
Aggressive supportive therapy
Successful neurologic recovery has been reported even after prolonged resuscitation in toxicologic arrests (Lavonas et al., 2023).
Antidotes During Resuscitation
Poisoning resuscitation incorporates toxin-specific therapies alongside standard ACLS medications.
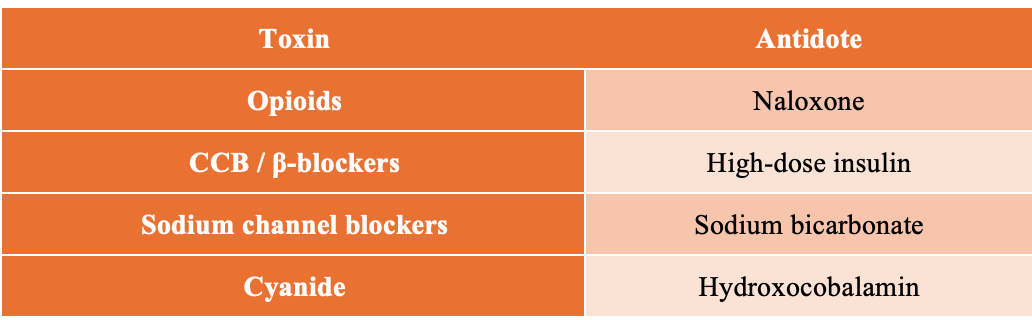
These therapies address the underlying mechanism of arrest, rather than simply supporting circulation.
Extracorporeal Life Support
Extracorporeal membrane oxygenation (ECMO) plays a particularly important role in toxicologic resuscitation.
Because poisoning often represents a reversible physiologic insult, ECMO may function as a bridge to toxin clearance and organ recovery (Ng et al., 2023).
Indications include:
Refractory toxic cardiogenic shock
Poisoning-related cardiac arrest
Severe cardiotoxic drug overdose.
When Should Resuscitation Stop?
Determining when to stop resuscitation is challenging in poisoning.
Delayed recovery may occur because:
Drugs have long half-lives
Sedatives delay neurologic recovery
Metabolites remain active
Therefore many toxicology experts recommend delayed prognostication and consultation with poison centers or toxicologists before withdrawal of care (Lavonas et al., 2023).
The Practical Emergency Medicine Takeaway
For emergency physicians, toxicologic resuscitation requires a shift in mindset.
Key principles include:
Apply standard ABCDE and ACLS frameworks.
Monitor physiologic trends rather than isolated values.
Use the ECG as an early diagnostic tool.
Initiate toxin-specific therapies early.
Consider detoxification strategies.
Be prepared for prolonged resuscitation.
Think of ECMO as a bridge to recovery rather than rescue therapy.
Because in toxicology:
What appears to be irreversible collapse may simply be physiology waiting for the toxin to clear.
References
Hüser N, et al. Management of poisoned patients in the emergency department: monitoring, risk stratification, and supportive care. Clinical Toxicology (Phila). 2025.
Lavonas EJ, Drennan IR, Gabrielli A, et al. 2023 American Heart Association focused update on toxicologic emergencies in cardiac arrest and resuscitation. Circulation. 2023;148(24):e___–e___.
Mégarbane B, Deye N, Bloch V, et al. Management of acute poisoning in intensive care: general principles and supportive care. Clinical Toxicology (Phila). 2020;58(6):487-502.
Bechtel LK, Holstege CP. Toxicologic testing in the emergency department: indications and limitations. Emergency Medicine Clinics of North America. 2022;40(2):345-360.
Ghannoum M, Roberts DM. Extracorporeal treatments in poisoning: indications and clinical applications. Clinical Journal of the American Society of Nephrology. 2023;18(3):467-479.
Ng PC, et al. Extracorporeal life support for poisoning and drug overdose. Circulation. 2023.
Vega RM, et al. Monitoring and early recognition of deterioration in poisoned patients. Clinical Toxicology (Phila). 2024.
Parris R, Calello DP. Initial approach to the poisoned patient in the emergency department. Emergency Medicine Clinics of North America. 2022;40(2):215-230.
Hoving S, et al. The ABCDE approach to the poisoned patient. Clinical Toxicology (Phila). 2011;49(6):517-524.
Ornillo TA, Harbord NB. Respiratory complications of poisoning and their management. Clinics in Chest Medicine. 2020;41(4):633-645.
Reyes JC, et al. Laboratory evaluation and risk stratification in acute poisoning. Clinical Toxicology (Phila). 2021.
El-Sarnagawy GN, et al. Clinical and laboratory predictors of outcomes in acute pediatric poisoning. Clinical Toxicology (Phila). 2023.
Elliott R, et al. Intraosseous access in emergency resuscitation. Resuscitation. 2017;121:1-6.
Upchurch CP, et al. Extracorporeal cardiopulmonary resuscitation in reversible causes of cardiac arrest. Circulation. 2021.
Von Ow D, Osterwalder J. Decontamination strategies in toxicologic emergencies. Clinical Toxicology (Phila). 2009.
Holstege CP, et al. Evaluation and management of the poisoned patient in critical care. Critical Care Clinics. 2008;24(1):103-119.
Pannu N. Toxicologic emergencies in the ICU: recognition and management. Critical Care Medicine. 2025.