

“The tube is in. Saturation is 99%. Blood pressure is stable. The procedure is over.”
Not quite.
By-
Dr Arihant Jain, MD | lifeonthefrontline.com
Instagram: @humans.of.em
X | Linkedin | ORCID
————————
One of the most preventable harms in emergency and critical care occurs after successful intubation—not during it. A patient receives induction with etomidate, ketamine, or propofol. A paralytic is administered. The airway is secured. The team celebrates a successful intubation.
But then the sedative wears off. The paralysis does not. For the next 30–60 minutes, the patient may be awake, aware, unable to move, unable to communicate, and unable to breathe independently.
Few experiences in medicine are more terrifying. Post-intubation sedation is not an optional intervention. It is the continuation of the intubation procedure itself.
The Goal Is Not Deep Sedation
Before discussing drugs, we must define the target.
Modern acute care has shifted away from routine deep sedation. Multiple studies have demonstrated that excessive sedation is associated with longer mechanical ventilation, increased delirium, prolonged ICU stays, and worse long-term outcomes.
For most mechanically ventilated patients, the target should be:
RASS -2 to 0
0 = Alert and calm
-1 = Drowsy
-2 = Light sedation
Patients should be comfortable, cooperative when appropriate, and free from pain—not chemically comatose.
Deep sedation (RASS -4 to -5) should be reserved for specific indications:
Severe ARDS requiring ventilator synchrony
Neuromuscular blockade
Refractory intracranial hypertension
Status epilepticus
Severe agitation threatening patient safety
The question is not “How deeply sedated can I make my patient?”, The question is “What is the lightest level of sedation that safely achieves my goals?”
This seemingly small shift in philosophy has transformed modern ICU practice.
You Can’t Target What You Don’t Measure
Post-intubation sedation, like shock resuscitation, must be goal-directed. (Baumgartner K, 2026)
Yet studies show sedation assessment in mechanically ventilated ED patients remains inconsistent, with documentation rates varying dramatically between institutions (Steel et al., 2021; Fuller et al., 2019).
Every intubated patient should have two explicit targets:
Pain target: Critical Care Pain Observation Tool (CPOT) if possible
Sedation target: Richmond Agitation-Sedation Scale (RASS), must
These assessments should be repeated regularly and tied to nursing-driven titration protocols. Because sedation is not a drug order. Consider it as a treatment target.
For most patients:
CPOT: As low as possible
RASS: -2 to 0
Without structured assessment, clinicians frequently default to over-sedation—a practice consistently associated with more delirium, longer ventilation, longer ICU stays, and higher mortality (Shehabi et al., 2012; Tanaka et al., 2014; Shehabi et al., 2018). What gets measured gets managed.
Sedation Begins the Moment the Tube Goes In
The most dangerous misconception after rapid sequence intubation is assuming that induction agents provide ongoing sedation. They do not. Typical durations are remarkably short:
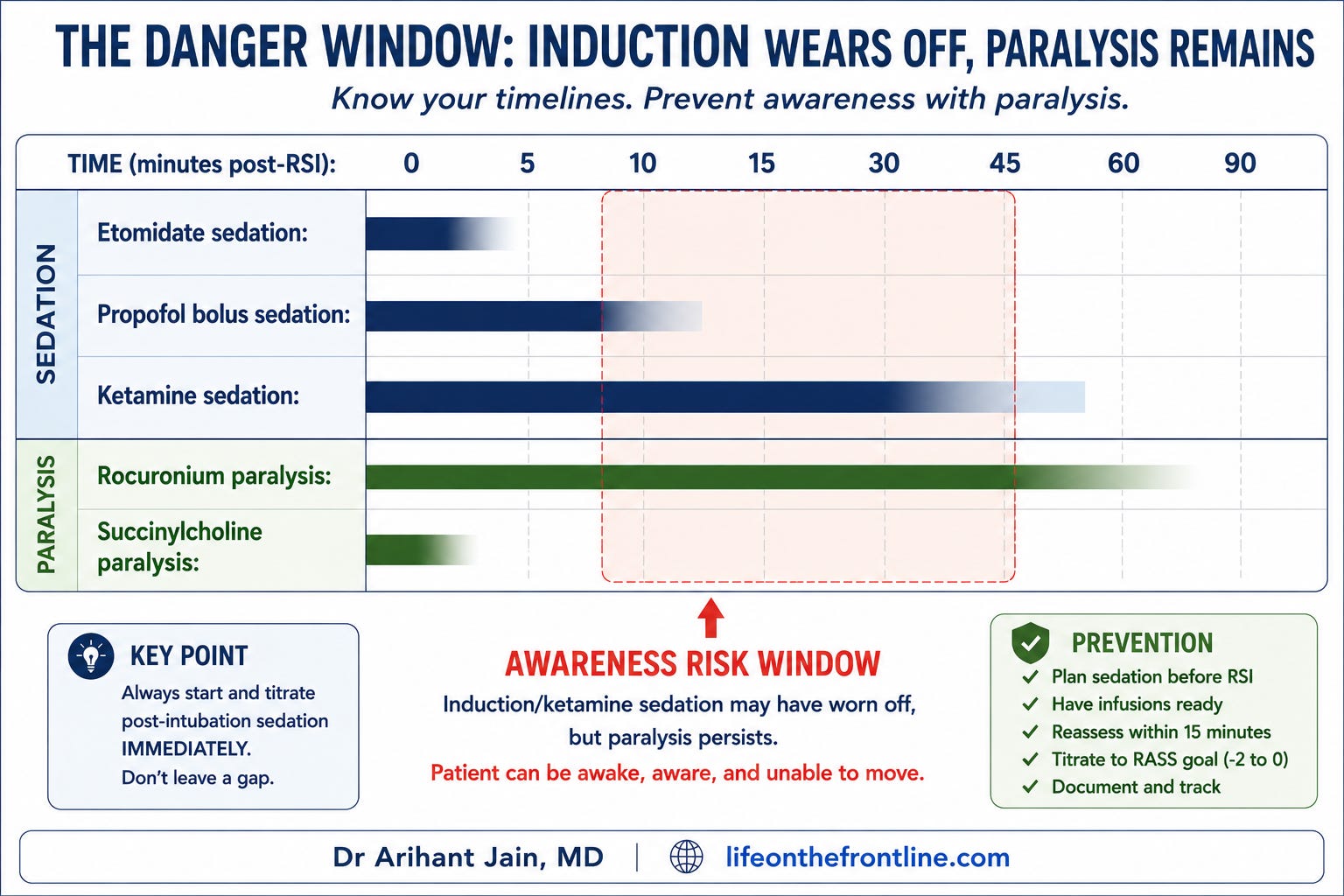
This creates a potentially devastating mismatch. The patient may regain awareness long before they regain movement. Every clinician who performs RSI should develop a habit:
Before the intubation begins, know what your post-intubation sedation plan will be.
Not afterward. Not when the chest X-ray returns. Not when the nurse reminds you. Before.
Awareness With Paralysis: The Complication We Don’t Measure Enough
Awareness during neuromuscular blockade is not rare. Prospective emergency department studies demonstrate unacceptably high rates of recall among mechanically ventilated patients (Pappal et al., 2021; Driver et al., 2023).
Risk factors include:
Rocuronium use
Delayed sedation initiation
Lack of sedation monitoring
Deeply sedated appearance masking inadequate analgesia
Patients who are paralyzed cannot demonstrate distress. Silence is not comfort.
The most effective prevention strategy is simple: Plan post-intubation sedation before intubation.
Build Sedation Into Your Airway Checklist
One of the simplest ways to prevent awareness with paralysis is to stop treating post-intubation sedation as an afterthought. Before administering induction drugs, ask:
“What is our sedation plan after the tube goes in?”
The answer should include:
Target RASS
Initial analgesic
Initial sedative
Vasopressor strategy if needed
Planned reassessment interval
Ideally, post-intubation medications should be prepared before laryngoscopy begins. (Baumgartner K, 2026). Multiple quality-improvement initiatives have shown that incorporating sedation into peri-intubation checklists reduces delays in analgesia and sedation initiation (Irwin et al., 2022; Ayers et al., 2024).
The patient should never wait for a chest radiograph, ICU bed assignment, or medication order reconciliation before receiving analgesia and sedation. Airway management does not end at endotracheal tube confirmation. It ends when the patient is comfortable.
The Rise—and Nuance—of Analgosedation
(Baumgartner K, 2026)
For decades, sedation-focused strategies dominated critical care. Patients received sedatives first, with analgesia added later if needed. Modern practice has shifted toward an analgesia-first philosophy.
Why?
Because many mechanically ventilated patients are not agitated because they need more sedation. They are agitated because they are in pain.
Pain increases:
Tachycardia
Hypertension
Ventilator dyssynchrony
Oxygen consumption
Agitation
Sedative requirements
Treating pain first often reduces the amount of sedative required. This approach is known as analgosedation.
However, post-intubation analgesia and sedation are linked—but distinct—interventions. (Baumgartner K, 2026)
Not every patient benefits from opioid escalation, and pain assessment can be challenging in critically ill, non-communicative patients. Current guidelines have softened earlier recommendations for strict analgesia-first approaches, emphasizing individualized care based on patient physiology and validated assessment tools (Devlin et al., 2018).
The practical message remains unchanged:
Do not mistake pain for a need for more sedation.
And do not mistake analgesia for sedation. Fentanyl may make patients more comfortable. It does not reliably make them unaware.
Fentanyl: The Most Misunderstood Drug in Post-Intubation Care
One concept deserves particular emphasis. Fentanyl is an analgesic. It is not primarily a sedative. This distinction is frequently misunderstood in emergency departments.
Mechanism
Fentanyl is a potent μ-opioid receptor agonist.
Its primary effects are:
Analgesia
Blunting of sympathetic responses
Reduction of pain-related agitation
At high doses, fentanyl can certainly contribute to sedation. However, sedation is not its principal therapeutic role.
Typical Dosing
Loading dose
25–100 mcg IV
Continuous infusion
25–200 mcg/hour
or approximately
0.5–3 mcg/kg/hour
Advantages
Rapid onset
Reliable analgesia
Familiarity
Minimal histamine release
Limitations
Respiratory depression
Chest wall rigidity with rapid high-dose administration
Drug accumulation during prolonged infusions
The practical takeaway is straightforward:
If your patient is receiving fentanyl alone, they may have excellent analgesia while remaining inadequately sedated.
Pain control and sedation are not synonymous.
Midazolam: The Old Workhorse
Midazolam remains one of the most commonly used sedatives worldwide.
Mechanism
Midazolam enhances GABA-A receptor activity, producing:
Sedation
Anxiolysis
Amnesia
Anticonvulsant effects
Typical Dosing
Loading
2–5 mg IV
Infusion
1–10 mg/hour
(approximately 0.02–0.1 mg/kg/hour)
When Midazolam Still Shines
Despite its declining popularity, midazolam remains valuable in:
Hemodynamically unstable patients
Status epilepticus
Alcohol withdrawal
Situations requiring profound amnesia
Deep sedation requirements
The Problem
The major issue with benzodiazepines is not inadequate sedation. It is excessive sedation.
Accumulation, particularly during prolonged infusions, contributes to:
Delayed awakening
Prolonged ventilation
Increased delirium
Longer ICU stays
Meta-analyses comparing midazolam with propofol and dexmedetomidine consistently demonstrate slower extubation and higher delirium rates with benzodiazepine-based strategies (Garcia et al., 2021; Chen & Ho, 2025).
Intermittent bolus doses of midazolam for breakthrough agitation are unlikely to carry the same risks as prolonged continuous infusions. The adverse outcome data are driven primarily by infusion-based benzodiazepine strategies.
For this reason, contemporary guidelines generally favor non-benzodiazepine sedatives whenever feasible.
Dexmedetomidine: Cooperative Sedation
If benzodiazepines represent traditional ICU sedation, dexmedetomidine represents the modern philosophy.
Mechanism
Dexmedetomidine is a selective alpha-2 adrenergic agonist. Unlike GABAergic sedatives, it produces a unique form of sedation. Patients often appear asleep but awaken easily and interact appropriately when stimulated.
Typical Dosing
Loading dose
Often omitted in critically ill patients due to hemodynamic effects.
Infusion
0.2–1.5 mcg/kg/hour
Advantages
Reduced delirium
Easier neurological assessment
Preserved respiratory drive
Improved patient interaction
Shorter time to extubation compared with benzodiazepines
Large meta-analyses demonstrate lower delirium rates and modest reductions in ventilation duration compared with traditional sedatives (Wen et al., 2023; Walsh et al., 2025).
Dexmedetomidine has a delayed onset. Without a loading dose, peak sedative effect may take 30–60 minutes. When rapid sedation is required, dexmedetomidine should be bridged with a faster-acting agent such as propofol.
Limitations
The trade-off is predictable:
Bradycardia
Hypotension
As with every sedative in critical care, benefits must be balanced against physiology.
Ketamine: More Than an Induction Agent
Most emergency physicians are comfortable using ketamine for induction.
Fewer use it as part of a post-intubation strategy.
Mechanism
Ketamine acts primarily through NMDA receptor antagonism.
Unlike most sedatives, it provides:
Analgesia
Sedation
Relative preservation of airway reflexes
Sympathomimetic effects
Typical Dosing
Loading
0.25–1 mg/kg
Infusion
0.1–2 mg/kg/hour
Where Ketamine Excels
Ketamine is particularly attractive in:
Severe bronchospasm
Opioid-tolerant patients
Hemodynamic instability
Patients requiring opioid-sparing strategies
Ketamine may be particularly useful in severe bronchospasm, polytrauma with difficult-to-control pain, refractory status epilepticus, or when propofol intolerance limits sedation options.
Recent reviews suggest ketamine’s greatest strength is as an adjunctive agent that reduces overall sedative and opioid requirements rather than as routine monotherapy (Hendrikse et al., 2023; Amer et al., 2024).
What About Propofol?
No discussion of post-intubation sedation would be complete without propofol. In many ICUs, propofol remains the default sedative.
Why?
Because it is:
Rapidly titratable
Predictable
Short acting
Associated with faster awakening and extubation
Typical dosing ranges from:
5–80 mcg/kg/min
Its major limitations are equally familiar:
Hypotension
Bradycardia
Hypertriglyceridemia
Propofol infusion syndrome (rare)
Compared with midazolam, propofol consistently shortens ventilation duration and accelerates extubation in mechanically ventilated patients (Garcia et al., 2021).
Propofol should be dosed using ideal body weight rather than actual body weight, particularly in obesity, to reduce the risk of hypotension. (Baumgartner K, 2026)
Rather than abandoning propofol when hypotension develops, clinicians should first consider reducing the infusion rate and initiating vasopressor support. Given its short duration of action, persistent hypotension despite dose reduction should prompt evaluation for alternative causes. (Baumgartner K, 2026)
For many patients, a combination of:
Fentanyl + Propofol
remains an excellent starting strategy.
This article focuses on emergency department management during the immediate post-intubation period. Sedation strategies should always be individualized based on patient physiology, institutional protocols, and evolving ICU goals.
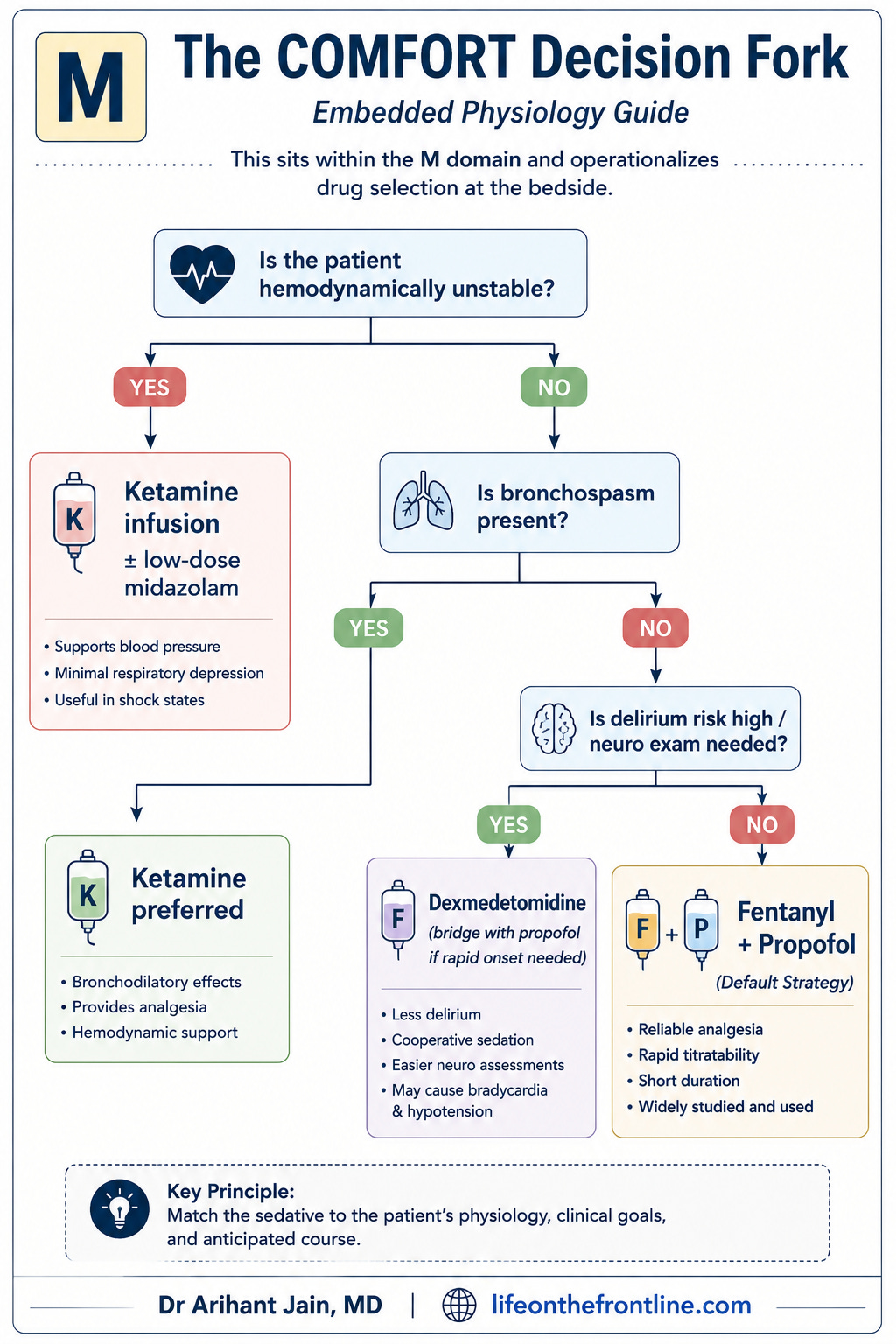
Choosing the Right Sedative
There is no universally superior sedative.
The best agent depends on the physiology in front of you. The goal is not to find the perfect drug. The goal is to match the drug to the patient.
The Bottom Line
The airway is not secured when the tube passes the cords.
The airway is secured when the patient is:
Adequately analgesed
Adequately sedated
Appropriately monitored
Maintained within a defined sedation target
Post-intubation sedation is not an afterthought.
It is not an ICU issue.
It is not something to “sort out later.”
It is a core component of airway management.
Because a patient who is awake, frightened, and paralyzed behind an endotracheal tube has not received complete care.
They have received an incomplete intubation.
References
Baumgartner K, Fuller BM. Postintubation sedation and analgesia in the emergency department: the basics and beyond. Emergency Medicine Clinics of North America. 2026. doi:10.1016/j.emc.2026.02.004.
Devlin JW, Skrobik Y, Gélinas C, et al. Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Critical Care Medicine. 2018;46(9):e825-e873. doi:10.1097/CCM.0000000000003299
Pandharipande PP, Girard TD, Jackson JC, et al. Long-term cognitive impairment after critical illness. New England Journal of Medicine. 2013;369(14):1306-1316. doi:10.1056/NEJMoa1301372
Shehabi Y, Bellomo R, Reade MC, et al. Early intensive care sedation predicts long-term mortality in ventilated critically ill patients. American Journal of Respiratory and Critical Care Medicine. 2012;186(8):724-731. doi:10.1164/rccm.201203-0522OC
Tanaka LMS, Azevedo LCP, Park M, et al. Early sedation and clinical outcomes of mechanically ventilated patients: a prospective multicenter cohort study. Critical Care. 2014;18(4):R156. doi:10.1186/cc13941
Shehabi Y, Bellomo R, Kadiman S, et al. Sedation intensity in the first 48 hours of mechanical ventilation and 180-day mortality: a multinational prospective longitudinal cohort study. Critical Care Medicine. 2018;46(6):850-859. doi:10.1097/CCM.0000000000003071
Boncyk C, Rolfsen M, Richards D, et al. Management of pain and sedation in the intensive care unit. BMJ. 2024;387:e079789. doi:10.1136/bmj-2024-079789
Garcia R, Salluh J, Andrade TR, et al. A systematic review and meta-analysis of propofol versus midazolam sedation in adult intensive care patients. Journal of Critical Care. 2021;64:91-99. doi:10.1016/j.jcrc.2021.04.001
Chen Y, Ho MH. Comparative risks and clinical outcomes of midazolam versus other intravenous sedatives in critically ill mechanically ventilated patients: a systematic review and meta-analysis of randomized trials. Intensive & Critical Care Nursing. 2025;103945. doi:10.1016/j.iccn.2025.103945
Wen J, Ding X, Liu C, et al. A comparison of dexmedetomidine and midazolam for sedation in patients with mechanical ventilation in ICU: a systematic review and meta-analysis. PLOS One. 2023;18:e0294292. doi:10.1371/journal.pone.0294292
Walsh TS, Parker RA, Aitken LM, et al. Dexmedetomidine- or clonidine-based sedation compared with propofol in critically ill patients: the A2B randomized clinical trial. JAMA. 2025. doi:10.1001/jama.2025.7200
Lewis K, Alshamsi F, Carayannopoulos K, et al. Dexmedetomidine versus other sedatives in critically ill mechanically ventilated adults: a systematic review and meta-analysis of randomized trials. Intensive Care Medicine. 2022;48:811-840. doi:10.1007/s00134-022-06712-2
Kawazoe Y, Miyamoto K, Morimoto T, et al. Effect of dexmedetomidine on mortality and ventilator-free days in patients requiring mechanical ventilation with sepsis: a randomized clinical trial. JAMA. 2017;317(13):1321-1328. doi:10.1001/jama.2017.2088
Hendrikse C, Ngah V, Kallon I, et al. Ketamine as adjunctive or monotherapy for post-intubation sedation in patients with trauma on mechanical ventilation: a rapid review. African Journal of Emergency Medicine. 2023;13:313-321. doi:10.1016/j.afjem.2023.10.002
Amer M, Møller MH, Alshahrani M, et al. Ketamine analgosedation for mechanically ventilated critically ill adults: a rapid practice guideline from the Saudi Critical Care Society and the Scandinavian Society of Anesthesiology and Intensive Care Medicine. Anesthesia & Analgesia. 2024. doi:10.1213/ANE.0000000000007173
Matchett G, Gasanova I, Riccio CA, et al. Continuous infusion ketamine for adjunctive analgosedation in mechanically ventilated, critically ill patients. Pharmacotherapy. 2019;39(3):288-296. doi:10.1002/phar.2223
Pappal RD, Roberts BW, Mohr NM, et al. The ED-AWARENESS study: a prospective observational cohort study of awareness with paralysis in mechanically ventilated patients admitted from the emergency department. Annals of Emergency Medicine. 2021;77(5):532-544. doi:10.1016/j.annemergmed.2020.09.026
Driver BE, Prekker ME, Wagner E, et al. Recall of awareness during paralysis among emergency department patients undergoing tracheal intubation. Chest. 2023;163(2):313-323. doi:10.1016/j.chest.2022.09.035
Fuller BM, Roberts BW, Mohr NM, et al. The ED-SED study: a multicenter, prospective cohort study of practice patterns and clinical outcomes associated with emergency department sedation for mechanically ventilated patients. Critical Care Medicine. 2019;47(11):1539-1548. doi:10.1097/CCM.0000000000003956
Fuller BM, Roberts BW, Mohr NM, et al. The feasibility of implementing targeted sedation in mechanically ventilated emergency department patients: the ED-SED pilot trial. Critical Care Medicine. 2022;50(8):1224-1235. doi:10.1097/CCM.0000000000005559
Steel TL, Lokhandwala S, Caldwell ES, et al. Variability in sedation assessment among intubated patients in the emergency department. Academic Emergency Medicine. 2021;28(10):1173-1176. doi:10.1111/acem.14329
Ely EW, Truman B, Shintani A, et al. Monitoring sedation status over time in ICU patients: reliability and validity of the Richmond Agitation-Sedation Scale. JAMA. 2003;289(22):2983-2991. doi:10.1001/jama.289.22.2983
Gélinas C, Fillion L, Puntillo KA, et al. Validation of the Critical-Care Pain Observation Tool in adult patients. American Journal of Critical Care. 2006;15(4):420-427.
Irwin WW, Berg KT, Ruttan T K, et al. Initiative to improve postintubation sedation in a pediatric emergency department. Journal for Healthcare Quality. 2022;44(1):31-39. doi:10.1097/JHQ.0000000000000304
Ayers C, Johnson DP, Noffsinger L, et al. Reducing time to postintubation sedation in a pediatric emergency department. Pediatrics. 2024;153(4):e2023062665. doi:10.1542/peds.2023-062665
This article synthesizes current evidence and recommendations from the 2018 SCCM PADIS Guidelines, recent emergency medicine literature, and the review by Baumgartner and Fuller (2026), “Postintubation Sedation and Analgesia in the Emergency Department: The Basics and Beyond.” It is intended for educational purposes and should complement—not replace—local protocols and clinical judgment.
👏🏽👏🏽👏🏽