
Platelet Transfusion ?
Why This Decision Makes Us Doubt Ourselves—and How to Get It Right

Platelet transfusion is one of the uncomfortable decisions we make in emergency and acute care.
Not because we don’t know the platelet count—but because the number rarely tells us what to do.
A patient with a platelet count of 18,000/µL looks stable.
Someone asks if platelets are needed “just in case.”
Another worries about a procedure, a bleed that hasn’t happened yet, or a complication no one wants to own.
And suddenly, an evidence-based decision turns into collective anxiety.
This uncertainty is not a failure of knowledge. It reflects how platelet transfusion has shifted—from a number-driven reflex to a context-driven intervention that demands judgment.
The Core Problem: Platelet Count ≠ Bleeding Risk
The platelet count is easy to measure, but it is a poor standalone predictor of bleeding, particularly in critically ill patients. Thrombocytopenia is common in the ED and ICU, yet clinically significant bleeding occurs in only a subset of patients (Pène et al., 2025).
Despite this, platelet transfusions remain frequent. Large audits show that 40–60% of adult platelet transfusions are guideline-discordant, most often given prophylactically at platelet counts well above evidence-based thresholds (Hill-Strathy et al., 2020; Russell et al., 2025).
In practice, we often transfuse to reduce discomfort—ours, not the patient’s.
ISTH Definition of Bleeding Severity
According to the International Society on Thrombosis and Haemostasis (ISTH):
Major bleeding is defined as any of the following:
Fatal bleeding
Symptomatic bleeding in a critical area or organ, including:
Intracranial
Intraspinal
Intraocular
Retroperitoneal
Intra-articular
Pericardial
Intramuscular bleeding with compartment syndrome
Bleeding associated with a fall in hemoglobin ≥20 g/L (1.24 mmol/L)
Bleeding requiring transfusion of ≥2 units of whole blood or red blood cells
Minor bleeding:
Any reported bleeding not meeting criteria for major bleeding
What the Evidence Actually Supports
Modern guidelines consistently endorse a restrictive, risk-adapted approach, rather than liberal transfusion based on platelet count alone (Kaufman et al., 2015; Estcourt et al., 2017; Metcalf et al., 2025).
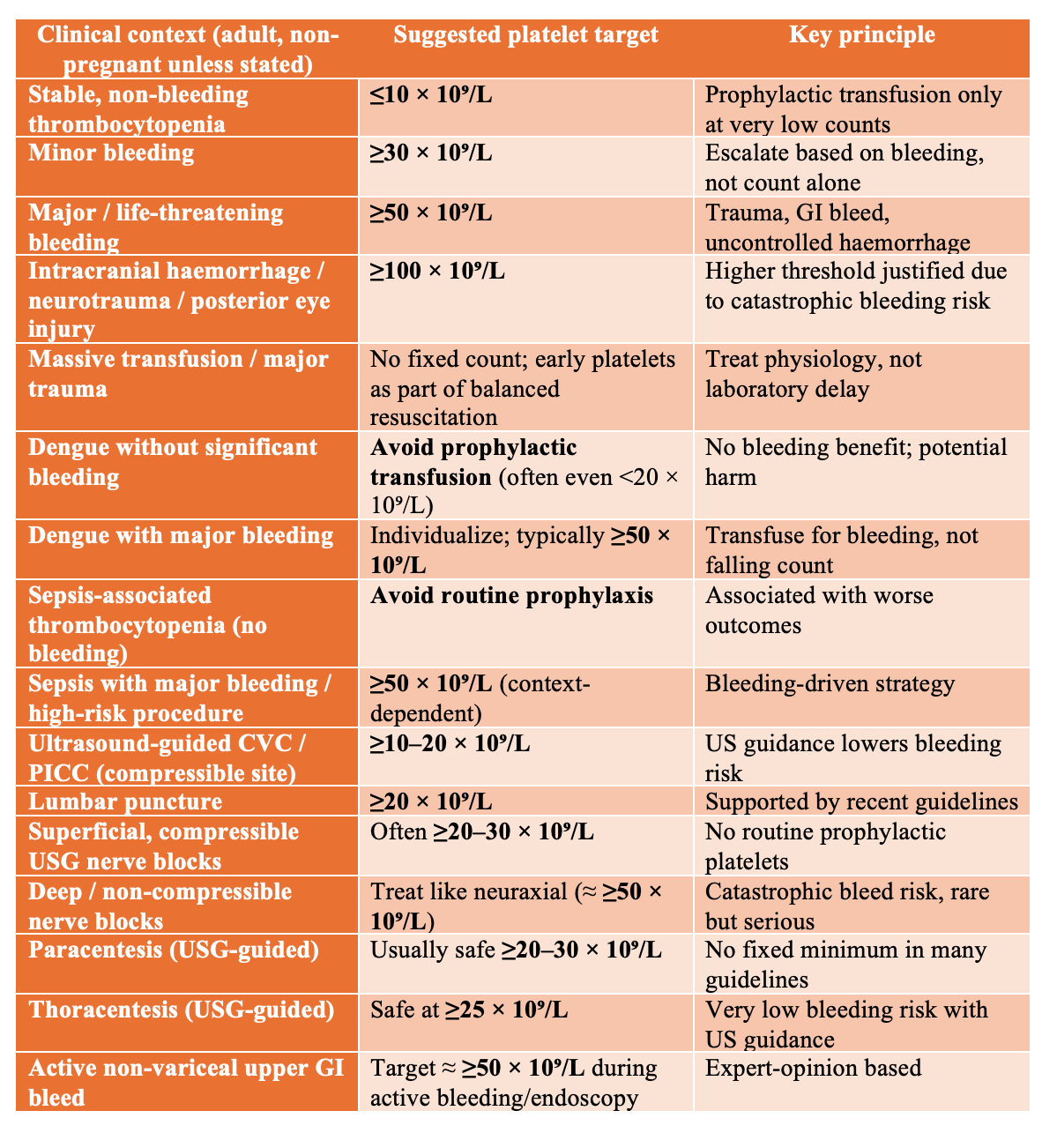
Non-bleeding patients
In stable adults with hypoproliferative thrombocytopenia and no bleeding, platelet transfusion is recommended only when counts fall to ≤10 × 10⁹/L. Transfusing above this threshold has not been shown to reduce bleeding or mortality (Kaufman et al., 2015; Kumar et al., 2015; Metcalf et al., 2025).
Bleeding patients
When bleeding is present, thresholds rise—but should remain proportional to severity:
Minor bleeding: often consider transfusion at <20 × 10⁹/L
Major or life-threatening bleeding : target ≥50 × 10⁹/L
Neurotrauma, posterior eye surgery, spinal injury: commonly ≥100 × 10⁹/L
(Pène et al., 2025; Estcourt et al., 2017; Metcalf et al., 2025)
Dengue and Sepsis: Low Counts, High Anxiety, Little Benefit
Few situations create more pressure to transfuse than dengue and sepsis-associated thrombocytopenia, where platelet counts fall rapidly but bleeding is often absent. In dengue, randomized trials and systematic reviews consistently demonstrate no benefit from prophylactic platelet transfusion in non-bleeding adults—even at counts below 20 × 10⁹/L—with no reduction in bleeding and frequent associations with adverse events, longer hospitalization, and delayed platelet recovery (Lye et al., 2009; Assir et al., 2013; Lye et al., 2017; Lee et al., 2016; Nakazaki & Cotera-Ramón, 2024).
Similarly, in sepsis, large ICU database analyses show that platelet transfusion is associated with higher 28- and 90-day mortality, without reductions in bleeding or transfusion requirements for other blood products (He et al., 2022; Pène et al., 2025). Current guidance therefore emphasizes a bleeding-guided, not count-guided strategy: treat the underlying illness, reserve platelets for clinically significant hemorrhage or clearly high-risk procedures, and avoid routine prophylaxis based on numbers alone (Metcalf et al., 2025; Yataco et al., 2025).
Procedures: Where Fear Drives Over-transfusion
Procedural anxiety accounts for a large proportion of unnecessary platelet transfusions in the ED.
High-quality data from ultrasound-guided central venous catheter placement—often used as a proxy for other low-risk procedures—show that serious bleeding is rare even with platelet counts between 10–50 × 10⁹/L, and that prophylactic platelet transfusion provides little clinical benefit (Van Baarle et al., 2023; Zarama et al., 2023).
For ultrasound-guided regional anesthesia, evidence supports an individualized approach. Superficial, compressible blocks can usually be performed safely at platelet counts around 20–30 × 10⁹/L in experienced hands, without routine transfusion, while deep, non-compressible blocks should be approached more cautiously and treated similarly to neuraxial procedures (Kinirons, 2019; Toscano et al., 2021).
Similarly, for paracentesis and thoracentesis, multiple series show no bleeding events with ultrasound guidance at platelet counts as low as 25–30 × 10⁹/L, challenging the dogma of a rigid 50 × 10⁹/L cutoff (Schildhouse et al., 2017; Biolato et al., 2023).
Procedure alone is not an indication for platelets.
Platelets Are Not Benign
Platelets are the most common blood component associated with transfusion reactions, including febrile reactions, allergic events, TRALI, infection risk, and volume overload (Stanworth & Shah, 2022; Jug et al., 2025).
More platelets do not mean more safety.
They often mean more harm—with no proven benefit.
Platelet targets in emergency care are best understood as ranges anchored to bleeding risk, not rigid numbers tied to anxiety or tradition.
Massive haemorrhage protocol (MHP) and trauma: platelets are necessary—but not unlimited
Early phase (uncontrolled haemorrhage):
In major trauma and massive haemorrhage, early platelet transfusion is appropriate as part of balanced resuscitation (approximately 1:1:1 with plasma and RBCs).
This approach improves early hemostasis and survival compared with crystalloid-heavy or RBC-dominant strategies (Johansson et al., 2014; Cannon et al., 2017).
Ongoing resuscitation:
After initial control, fixed ratios should give way to goal-directed therapy.
Viscoelastic testing (TEG/ROTEM)–guided transfusion reduces unnecessary platelet and plasma use while improving survival compared with conventional lab-guided or purely ratio-based protocols (Gonzalez et al., 2016; Stein et al., 2017; Nunns et al., 2018).
Platelet targets in trauma:
Aim for ≥50 × 10⁹/L during active hemorrhage.
In traumatic brain injury or CNS involvement, higher targets (≈ ≥100 × 10⁹/L) are reasonable due to catastrophic bleeding risk.
Outside of active bleeding, routine “top-up” platelet transfusion is not supported.
Key principles: restrictive and goal-directed platelet transfusion
Restrictive platelet strategies are as safe as liberal strategies across most clinical settings, with no increase in bleeding or mortality and fewer transfusion-related harms (Metcalf et al., 2025; Stanworth & Shah, 2022; Jug et al., 2025).
Liberal prophylactic transfusion—especially in non-bleeding patients—has no proven benefit and may increase complications, including transfusion reactions, lung injury, and inflammatory effects.
Modern guidance consistently favors context-specific thresholds, integrating bleeding severity, procedure risk, and clinical trajectory rather than platelet count alone.
Bleeding severity matters: anchoring decisions to outcomes
Transfusion decisions should be framed around clinically meaningful bleeding, not laboratory abnormalities.
Using standardized definitions—such as ISTH major bleeding (fatal bleeding, bleeding in critical organs, Hb fall ≥20 g/L, or need for ≥2 units of RBCs)—helps align platelet use with outcomes that actually matter to patients.
Minor bleeding, by contrast, rarely justifies aggressive platelet correction in the absence of other high-risk features.
A Practical ED Mental Model
Instead of asking “What’s the platelet count?”, consider:
Is the patient actively bleeding?
Is the procedure truly high risk and non-compressible?
Am I transfusing for evidence—or for reassurance?
In massive haemorrhage and trauma, early platelet transfusion as part of balanced resuscitation is appropriate and lifesaving (Sperry et al., 2024). Outside of that context, restraint is usually the safer choice.
Disclaimer !!!
This post is intended for educational purposes only. It is not a substitute for professional medical advice, clinical judgment, or institutional protocols. Clinical decisions regarding platelet transfusion should always be individualised based on patient-specific factors, local guidelines, and real-time clinical context.
References
Kaufman RM, Djulbegovic B, Gernsheimer T, et al. Platelet transfusion: a clinical practice guideline from the AABB. Ann Intern Med. 2015;162(3):205-213. doi:10.7326/M14-1589
Metcalf R, Nahirniak S, Guyatt G, et al. Platelet transfusion: 2025 AABB and ICTMG international clinical practice guidelines. JAMA. 2025;334(2):156-168. doi:10.1001/jama.2025.7529
Estcourt LJ, Birchall J, Allard S, et al. Guidelines for the use of platelet transfusions. Br J Haematol. 2017;176(3):365-394. doi:10.1111/bjh.14423
Kumar A, Mhaskar R, Grossman BJ, et al. Platelet transfusion: a systematic review of the clinical evidence. Transfusion. 2015;55(5):1116-1127. doi:10.1111/trf.12943
Stanworth SJ, Shah A. How I use platelet transfusions. Blood. 2022;140(8):826-834. doi:10.1182/blood.2022016558
Hill-Strathy M, Pinkerton PH, Thompson T, et al. Evaluating the appropriateness of platelet transfusions compared with evidence-based platelet guidelines. Transfusion. 2021;61(1):57-71. doi:10.1111/trf.16134
Russell L, Azoulay É, Anthon C, et al. Platelet transfusion practice in the intensive care unit: the Nine-I international survey. Ann Intensive Care. 2025;15:94. doi:10.1186/s13613-025-01494-4
Pène F, Russell L, Aubron C. Thrombocytopenia in the intensive care unit: diagnosis and management. Ann Intensive Care. 2025;15:87. doi:10.1186/s13613-025-01447-x
Dengue and Sepsis
Lye DC, Lee VJ, Sun Y, Leo YS. Lack of efficacy of prophylactic platelet transfusion for severe thrombocytopenia in adults with acute uncomplicated dengue infection. Clin Infect Dis. 2009;48(9):1262-1265. doi:10.1086/597773
Assir MZ, Kamran U, Ahmad HI, et al. Effectiveness of platelet transfusion in dengue fever: a randomized controlled trial. Transfus Med Hemother. 2013;40(5):362-368. doi:10.1159/000354837
Lye DC, Archuleta S, Syed-Omar SF, et al. Prophylactic platelet transfusion versus supportive care in adults with dengue and thrombocytopenia. Lancet. 2017;389(10079):1611-1618. doi:10.1016/S0140-6736(17)30269-6
Lee TH, Wong JGX, Leo YS, et al. Potential harm of prophylactic platelet transfusion in adult dengue patients. PLoS Negl Trop Dis. 2016;10(3):e0004576. doi:10.1371/journal.pntd.0004576
Nakazaki J, Cotera-Ramón A. Assessment of the importance of platelet transfusion in patients with severe dengue: a systematic review. Iberoam J Med. 2024. doi:10.53986/ibjm.2024.0010
He S, Fan C, Tang C, Chen Y. Platelet transfusion in patients with sepsis and thrombocytopenia: a propensity score–matched analysis. Front Med (Lausanne). 2022;9:830177. doi:10.3389/fmed.2022.830177
Yataco A, Soghier I, Hébert P, et al. Transfusion of fresh frozen plasma and platelets in critically ill adults. Chest. 2025;168(2):661-676. doi:10.1016/j.chest.2025.02.029
Procedures, USG, Regional Anesthesia
Van Baarle FEH, Van de Weerdt EK, et al. Platelet transfusion before central venous catheter placement in patients with thrombocytopenia. N Engl J Med. 2023;388(21):1956-1965. doi:10.1056/NEJMoa2214322
Zarama V, Revelo-Noguera J, Quintero J, et al. Prophylactic platelet transfusion and bleeding risk with ultrasound-guided central venous access. Acad Emerg Med. 2023;30(6):644-652. doi:10.1111/acem.14651
Kinirons B. Peripheral nerve block in the patient with haemostatic disorder. Reg Anesth Pain Med. 2019;44(Suppl 1):A46-A48. doi:10.1136/rapm-2019-ESRAABS2019.45
Toscano A, Capuano P, Galatà M, et al. Safety of ultrasound-guided fascial plane blocks in patients on antithrombotic therapy. J Cardiothorac Vasc Anesth. 2021;35(11):3226-3232. doi:10.1053/j.jvca.2021.05.037
Schildhouse RJ, Lai A, Barsuk JH, et al. Safe and effective bedside thoracentesis: a review of the evidence. J Hosp Med. 2017;12(4):266-276. doi:10.12788/jhm.2716
Biolato M, Vitale F, Galasso T, et al. Minimum platelet count threshold before invasive procedures in cirrhosis. World J Gastrointest Surg. 2023;15(2):127-141. doi:10.4240/wjgs.v15.i2.127
ISTH Bleeding Definitions
Schulman S, Kearon C; Subcommittee on Control of Anticoagulation of the International Society on Thrombosis and Haemostasis. Definition of major bleeding in clinical investigations of antihemostatic medicinal products. J Thromb Haemost. 2005;3(4):692-694. doi:10.1111/j.1538-7836.2005.01204.x
Trauma, MHP, and Goal-Directed Transfusion
Johansson PI, Stensballe J, Oliveri R, et al. How I treat patients with massive hemorrhage. Blood. 2014;124(20):3052-3058. doi:10.1182/blood-2014-05-575340
Cannon JW, Khan MA, Raja AS, et al. Damage control resuscitation in patients with severe traumatic hemorrhage. J Trauma Acute Care Surg. 2017;82(3):605-617. doi:10.1097/TA.0000000000001333
Gonzalez E, Moore EE, Moore HB, et al. Goal-directed hemostatic resuscitation of trauma-induced coagulopathy. Ann Surg. 2016;263(6):1051-1059. doi:10.1097/SLA.0000000000001608
Stein P, Kaserer A, Sprengel K, et al. Change of transfusion and treatment paradigm in major trauma patients. Anaesthesia. 2017;72(11):1317-1326. doi:10.1111/anae.13920
Nunns GR, Moore EE, Stettler GR, et al. Empiric transfusion strategies during life-threatening hemorrhage. Surgery. 2018;164(2):306-311. doi:10.1016/j.surg.2018.02.024
Sperry JL, Guyette FX, Rosario-Rivera BL, et al. Early cold-stored platelet transfusion following severe injury. Ann Surg. 2024;280(2):212-221. doi:10.1097/SLA.0000000000006317
Jug R, La Rocca U, Al-Riyami A, et al. The clinical use of platelet transfusions: a systematic review and meta-analysis. Transfusion. 2025;65(6):1155-1169. doi:10.1111/trf.18277