

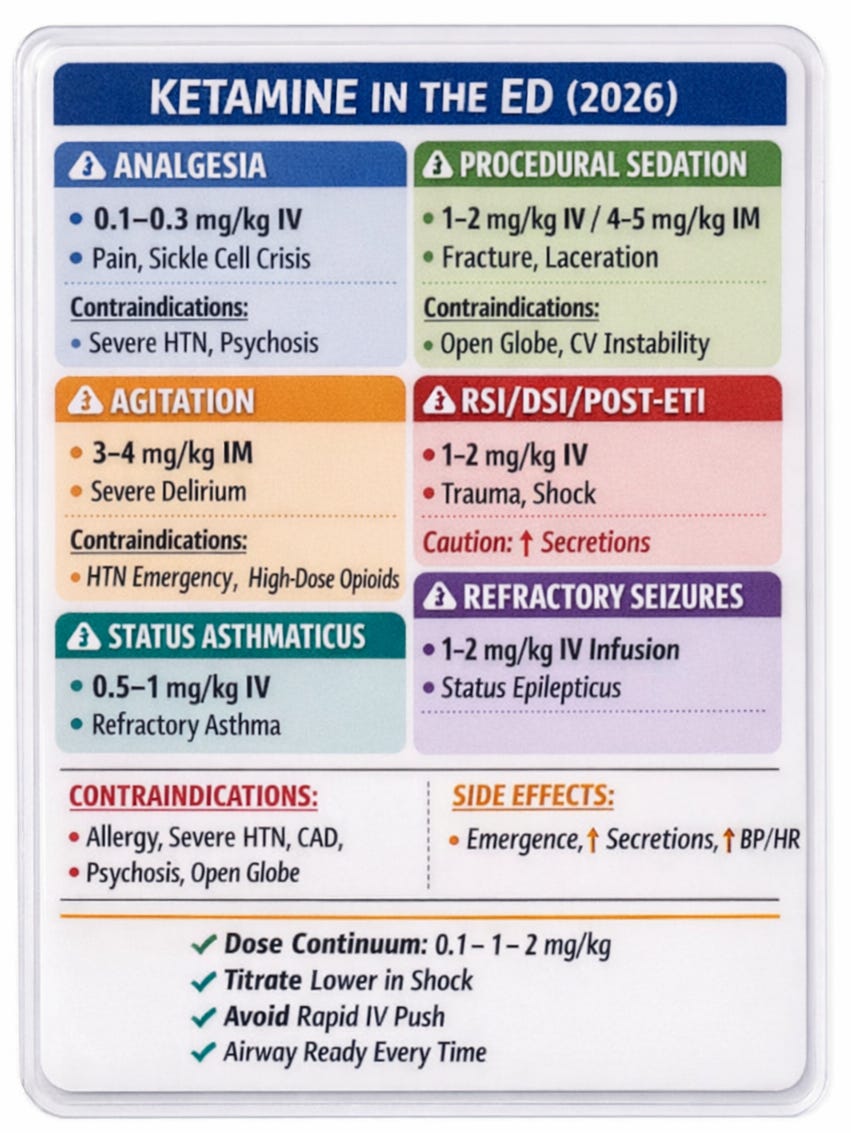
Ketamine remains one of the most versatile agents in emergency medicine, spanning analgesia, procedural sedation, agitation control, bronchodilation, refractory seizures, and airway management. Recent ED literature and updated dosing guidance (Engstrom et al., 2025; Green et al., 2025; Mirfazaelian et al., 2025) reinforce a dose-dependent continuum approach rather than viewing ketamine as a single-indication drug.
1️⃣ Ketamine for Acute Pain (Sub-dissociative Dosing)
IV Analgesia
0.1–0.3 mg/kg IV infusion over 15–30 min
Repeat in 1–2 hours if needed
Consider infusion 0.05–0.25 mg/kg/h for ongoing pain
(Engstrom et al., 2025)Ketamine _ CorePendium
What’s new:
Recent ED trials confirm that ~0.3 mg/kg IV provides comparable analgesia to opioids with fewer respiratory events (Beaudrie-Nunn et al., 2023; Lovett et al., 2020). Infusion is preferred over rapid IV push to reduce dizziness and psychoperceptual effects (Engstrom et al., 2025)
Alternative Routes
Intranasal: 0.75–1 mg/kg
Nebulized: 0.75–1 mg/kg
(Engstrom et al., 2025)Ketamine _ CorePendium
Clinical Pearl: Excellent option when IV access is delayed (pediatrics, trauma, behavioral emergencies).
2️⃣ Procedural Sedation (PSA)
IV Dissociative Sedation
1 mg/kg IV, repeat 0.5 mg/kg as needed
(Engstrom et al., 2025)Ketamine _ CorePendium
IM Dissociation
4–5 mg/kg IM
Repeat 2–5 mg/kg if required
(Engstrom et al., 2025)Ketamine _ CorePendium
Pediatric Safety Update
Large pediatric ED registry: critical AEs 0.016%
Meta-analysis (8,282 children): airway events increase with ≥2.5 mg/kg IV initial dose or ≥5 mg/kg total dose
(Green et al., 2009; Green et al., 2025)
Emerging trend (2024–2025):
Moderate dosing (0.5–1 mg/kg IV) achieves adequate sedation with fewer adverse effects than higher dosing (Türkücü et al., 2025).
Structured sedation programs significantly reduce complications (Erumbala et al., 2023).
3️⃣ Acute Agitation & Behavioral Emergencies
IM for Severe Agitation
3–4 mg/kg IM initial agent
2 mg/kg IM if adjunctive or sedative intoxication
(Engstrom et al., 2025)Ketamine _ CorePendium
IV (if access available)
1–2 mg/kg IV (less well studied for agitation)
Key Updates:
ED airway intervention rates are significantly lower than early EMS reports when dosing is standardized (Mankowitz et al., 2018; Kwong et al., 2025).
Avoid polypharmacy with opioids or benzodiazepines unless clinically indicated — airway events increase with co-administration.
4️⃣ Airway Management: RSI, DSI & Post-Intubation
RSI Induction
1–2 mg/kg IV push
In shock: 0.5–1 mg/kg IV, titrate
(Engstrom et al., 2025)
Delayed Sequence Intubation (DSI)
~1 mg/kg IV to achieve dissociation while preserving respirations
(Merelman et al., 2019)
Post-Intubation Sedation
Bolus 1–2 mg/kg
Infusion 1–5 mg/kg/h
Hemodynamic Advantage:
Ketamine supports blood pressure via indirect sympathomimetic activity (Engstrom et al., 2025)
Important nuance (2025 update):
Higher induction doses (2 mg/kg) in shock have been associated with post-intubation hypotension — titrated dosing (0.5 mg/kg increments) is recommended
5️⃣ Status Asthmaticus
Non-intubated
0.5–1 mg/kg IV bolus
0.25–0.5 mg/kg/h infusion
Intubated
Up to 0.75–3 mg/kg/h infusion
Bronchodilation is clinically useful, though meta-analyses show mixed outcome benefit (Engstrom et al., 2025)
6️⃣ Refractory Status Epilepticus
1–2 mg/kg IV bolus
0.1–4 mg/kg/h infusion
Continuous EEG recommended
(Engstrom et al., 2025)
Ketamine’s NMDA antagonism is particularly valuable in late-phase refractory seizures.
7️⃣ Special Populations & Safety Pearls
Pregnancy
Should not be withheld if clinically indicated
Single ED dose unlikely to cause fetal harm
(Engstrom et al., 2025)
Breastfeeding
Avoid for 6–12 hours post-dose
Intracranial Pressure
Contemporary data suggest ketamine does not increase ICP and may reduce it.
Adverse Effects to Anticipate
Emergence reactions (10–20%)
Laryngospasm - < 3 months (rare; manage with Larson maneuver)
Increased secretions (consider glycopyrrolate 0.2 mg IV)
Nausea/vomiting
📌 2026 Clinical Takeaways
Think in a dose continuum — analgesia (0.1 mg/kg) → dissociation (1 mg/kg) → airway control (1–2 mg/kg).
Moderate IV dosing (0.5–1 mg/kg) often balances efficacy and safety for PSA.
In shock, titrate (0.5 mg/kg increments) rather than reflexively giving 2 mg/kg.
Avoid unnecessary co-administration of respiratory depressants.
Pediatric safety remains excellent when high doses are avoided.
Ketamine remains one of the most hemodynamically stable induction agents in ED airway management.
References
Mirfazaelian H, Fazel A, Azizi N, et al. Non-injectable ketamine for pediatric sedation in the emergency department: a systematic review. Acad Emerg Med. 2025;32:1344-1355. doi:10.1111/acem.70163
Sharif S, Kang J, Sadeghirad B, et al. Pharmacological agents for procedural sedation and analgesia in the emergency department and intensive care unit: a systematic review and network meta-analysis of randomized trials. Br J Anaesth. 2024. doi:10.1016/j.bja.2023.11.050
Esmaillian M, Kouhestani S, Azizkhani R, et al. Dexmedetomidine versus propofol: an effective combination with ketamine for adult procedural sedation: a randomized clinical trial. Am J Emerg Med. 2023;73:95-101. doi:10.1016/j.ajem.2023.08.025
Türkücü Ç, Parlak I, Kokulu K, Sert E, Mutlu H. Comparison of the incidence of recovery agitation with two different doses of ketamine in procedural sedation: a randomized clinical trial. Acad Emerg Med. 2025;32:857-862. doi:10.1111/acem.15116
Ghojazadeh M, Sanaie S, Paknezhad S, et al. Using ketamine and propofol for procedural sedation of adults in the emergency department: a systematic review and meta-analysis. Adv Pharm Bull. 2019;9:5-11. doi:10.15171/apb.2019.002
De Vries L, Veeger N, Van Roon E, Lameijer H. Low-dose ketamine or opioids combined with propofol for procedural sedation in the emergency department: a systematic review. Eur J Emerg Med. 2023;30:244-251. doi:10.1097/MEJ.0000000000001046
Nasir H, Zahid M, Saleh M, et al. Use of ketamine, propofol and their combination (ketofol) for procedural sedation in emergency department: a review. Pak J Health Sci. 2023;4(02). doi:10.54393/pjhs.v4i02.539
Poonai N, Canton K, Ali S, et al. Intranasal ketamine for procedural sedation and analgesia in children: a systematic review. PLoS One. 2017;12:e0173253. doi:10.1371/journal.pone.0173253
Jamal D, Powell C. Paediatric procedural sedation in the emergency department: is ketamine safe? Arch Dis Child. 2020;106:120-124. doi:10.1136/archdischild-2019-318610
Dilip T, Chandy G, Hazra D, et al. The adverse effects of ketamine on procedural sedation and analgesia in the emergency department. J Fam Med Prim Care. 2021;10:2279-2283. doi:10.4103/jfmpc.jfmpc_2140_20
M S, S J, A B, et al. A randomized controlled trial comparing ketamine versus fentanyl for procedural sedation in the emergency department for adults with isolated extremity injury. Malays Orthop J. 2024;18:116-124. doi:10.5704/moj.2403.015
Elsaeidy A, Ahmad A, Kohaf N, et al. Efficacy and safety of ketamine-dexmedetomidine versus ketamine-propofol combination for periprocedural sedation: a systematic review and meta-analysis. Curr Pain Headache Rep. 2024;28:211-227. doi:10.1007/s11916-023-01208-0
Anoumandane A, Murugesan V, Jayabalan K, et al. Comparison of ketamine-dexmedetomidine and ketamine-propofol for procedural sedation in adults – a single-center prospective randomized control study. Asian J Med Sci. 2025. doi:10.71152/ajms.v16i10.4770
Dehne L, Foertsch M, Bradshaw P, et al. Evaluation of subdissociative-dose ketamine for procedural sedation in the emergency department. Crit Care Med. 2022. doi:10.1097/01.ccm.0000908972.43680.39
Rached-d’Astous S, Finkelstein Y, Bailey B, et al. Intranasal ketamine for procedural sedation in children: an open-label multicenter clinical trial. Am J Emerg Med. 2023;67:10-16. doi:10.1016/j.ajem.2023.01.046
Erumbala G, Anzar S, Deiratany S, et al. Procedural sedation programme minimising adverse events: a 3-year experience from a tertiary paediatric emergency department. Arch Dis Child. 2023;109:88-92. doi:10.1136/archdischild-2023-326021
Strayer RJ, Nelson LS. Adverse events associated with ketamine for procedural sedation in adults. Am J Emerg Med. 2008;26:985-1028. doi:10.1016/j.ajem.2007.12.005
Green SM, Roback MG, Krauss B, et al. Predictors of airway and respiratory adverse events with ketamine sedation in the emergency department: an individual-patient data meta-analysis of 8,282 children. Ann Emerg Med. 2009;54:158-168.e1-4. doi:10.1016/j.annemergmed.2008.12.011
Green SM, Tsze DS, Roback MG. Emergency department ketamine sedation: frequency and predictors of critical and high-risk adverse events. Ann Emerg Med. 2025. doi:10.1016/j.annemergmed.2025.05.003
White N, Wendt W, Drendel A, Walsh P. Sedation with ketamine, propofol, and dexmedetomidine in pediatric emergency departments. Am J Emerg Med. 2025;93:21-25. doi:10.1016/j.ajem.2025.03.027
Merelman AH, Perlmutter MC, Strayer RJ. Alternatives to rapid sequence intubation: contemporary airway management with ketamine. West J Emerg Med. 2019;20:466-471. doi:10.5811/westjem.2019.4.42753
Mankowitz SL, Regenberg P, Kaldan J, Cole JB. Ketamine for rapid sedation of agitated patients in the prehospital and emergency department settings: a systematic review and proportional meta-analysis. J Emerg Med. 2018;55:670-681. doi:10.1016/j.jemermed.2018.07.017
Kwong J, Verbeek PR, Leong Y, et al. Paramedic use of ketamine for severe agitation and violence. Can J Emerg Med. 2025;27:653-660. doi:10.1007/s43678-025-00963-w
Beaudrie-Nunn A, Wieruszewski E, Woods E, et al. Efficacy of analgesic and sub-dissociative dose ketamine for acute pain in the emergency department. Am J Emerg Med. 2023;70:133-139. doi:10.1016/j.ajem.2023.05.026
Lovett S, Reed T, Riggs R, et al. A randomized, noninferiority, controlled trial of two doses of intravenous subdissociative ketamine for analgesia in the emergency department. Acad Emerg Med. 2020;28. doi:10.1111/acem.14200
Engstrom K, Nordt SP, Acquisto NM, Won K, Rech MA, Swadron S, Mattu A. Ketamine. In: CorePendium. EM:RAP; Updated August 2, 2025.
Ketamine _ CorePendium
👏🏽👏🏽👏🏽