
Hypertonic Saline vs Mannitol : What We Prefer Less Often Matters More Than What We Prefer
A practical, evidence-based update for emergency & acute care clinicians

The debate over hypertonic saline (HTS) vs mannitol for reducing intracranial pressure (ICP) has gone on for years — and the truth is, the preferred agent remains controversial.
But here’s what’s NOT controversial:
➡️ We clearly know when not to use one.
➡️ And in the ED, those contraindications matter more than theoretical superiority.
Both agents work. Both reduce ICP. But their safety profiles, contraindications, and dosing nuances are the real decision-makers.
This article focuses on the evidence that your shift actually needs:
Which one works better when
Who should never get one or the other
Practical bedside dosing (adults + paediatrics)
Sodium & osmolality cutoff values
Updated literature you can trust
1. Efficacy & Safety: What the Evidence Really Shows
Both work — but hypertonic saline often performs better in the sickest patients.
Across RCTs and meta-analyses:
HTS is as effective or superior to mannitol
HTS shows better ICP reduction in refractory or severe TBI
HTS is especially beneficial in:
✔ unstable hemodynamics
✔ paediatric CNS infections
✔ dehydration
✔ renal compromise
(Gu et al., 2018; Mangat et al., 2019; Ashraf et al., 2024; Kamel et al., 2011; Rameshkumar et al., 2020; Hemmati et al., 2025)
Safety: HTS has fewer problems than mannitol
Hypertonic Saline advantages
More stable blood pressure
Less renal injury
No over-diuresis
Fewer electrolyte swings
Can be used when hypotensive
Mannitol risks
Hypotension
Hypovolemia
Renal failure
Rebound ICP
Dilutional hyponatremia
(Ashraf, 2024; Kamel, 2011; Kumar, 2024)
Patient Outcomes
Outcomes like mortality and neurological recovery are similar, but:
➡️ HTS may reduce ICU stay and ventilator duration.
(Ashraf, 2024; Karamian, 2024)
2. Absolute Contraindications (The REAL Deciding Factor)
Agent
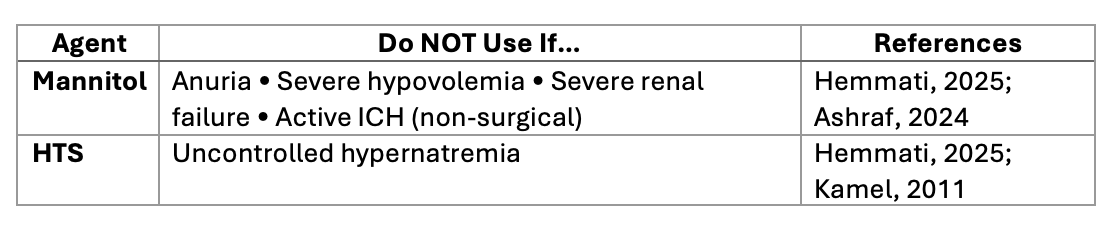
This is the cleanest bedside rule:
—> If the patient is dehydrated, hypotensive, or renally compromised → avoid mannitol.
—>If sodium is already high or the patient is in heart failure → avoid HTS.
3. Serum Sodium & Osmolality Cutoffs (Critical Numbers)
Mannitol
Absolute contraindication: Serum osmolality >320 mOsm/L
Avoid in severe hyponatremia
(Fink, 2012; Park & Ko, 2023)
Hypertonic Saline
Avoid if serum sodium >160–165 mEq/L
Caution if osmolality >320–350 mOsm/L
(Fink, 2012; Shao, 2015)
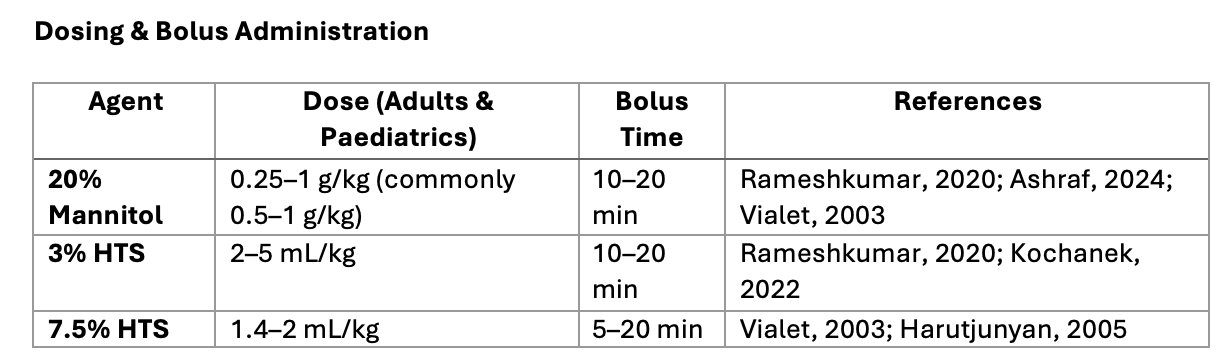
4. Practical Bedside Doses (Adults & Paediatrics)
Clinical Notes
3% HTS can be given peripherally if monitored (Khasiyev, 2024).
Higher concentrations → central line preferred.
Repeat boluses or infusions depend on ICP response & protocols.
5. Key Takeaways for Busy ED Clinicians
✔ Both agents work — but HTS is safer in high-risk patients
✔ Mannitol should NOT be used above 320 mOsm/kg
✔ HTS should NOT be used above Na 160–165 mEq/L
✔ Dosing is similar in adults & paediatrics
✔ The real ED decision is guided by contraindications, NOT preference
✔ HTS may outperform mannitol in refractory ICP
Bottom line:

References
1. Rameshkumar et al., 2020
Randomized Clinical Trial of 20% Mannitol vs 3% HTS in Children With Raised ICP. Pediatric Critical Care Medicine, 21:1071–1080.
https://doi.org/10.1097/pcc.0000000000002557
2. Ashraf et al., 2024
Comparison of Mannitol vs HTS for ICP Management. Biological and Clinical Sciences Research Journal.
https://doi.org/10.54112/bcsrj.v2024i1.1010
3. Gu et al., 2018
Meta-analysis: HTS vs Mannitol in TBI. Neurosurgical Review, 42:499–509.
https://doi.org/10.1007/s10143-018-0991-8
4. Kamel et al., 2011
Meta-analysis of HTS vs Mannitol. Critical Care Medicine, 39:554–559.
https://doi.org/10.1097/ccm.0b013e318206b9be
5. Hemmati et al., 2025
Systematic Review: Complications of HTS vs Mannitol.
https://doi.org/10.1101/2025.04.25.25326424
6. Kochanek et al., 2022
ICP Response to HTS vs Mannitol in Severe Pediatric TBI. JAMA Network Open, 5.
https://doi.org/10.1001/jamanetworkopen.2022.0891
7. Harutjunyan et al., 2005
RCT comparing 7.2% HTS HES vs 15% Mannitol in Neurosurgery. Critical Care, 9:R530–R540.
https://doi.org/10.1186/cc3767
8. Mangat et al., 2019
HTS superior to Mannitol for ICP & CPP burden. Neurosurgery.
https://doi.org/10.1093/neuros/nyz046
9. Alfarhan et al., 2023
HTS vs Mannitol in Children: Systematic Review.
https://doi.org/10.5742/mewfm.2023.95256187
10. Kumar et al., 2024
20% Mannitol vs 3% HTS in Non-Traumatic ICP: Meta-analysis. Indian J Crit Care Med, 28:686–695.
https://doi.org/10.5005/jp-journals-10071-24746
11. Susanto & Riantri, 2022
Optimal HTS Dose & Concentration in TBI. Medeniyet Medical Journal, 37:203–211.
https://doi.org/10.4274/mmj.galenos.2022.75725
12. Karamian et al., 2024
Systematic Review: HTS vs Mannitol in severe TBI. Neurological Research, 46:883–892.
https://doi.org/10.1080/01616412.2024.2360862
13. Huang et al., 2020
Equimolar Hypertonic Agents for ICP. Medicine, 99.
https://doi.org/10.1097/md.0000000000022004
14. Vialet et al., 2003
7.5% HTS vs 20% Mannitol in Refractory ICP. Critical Care Medicine, 31:1683–1687.
https://doi.org/10.1097/01.ccm.0000063268.91710.df
15. James, 2005
Methodology for ICP control using mannitol. Acta Neurochirurgica, 51:161–172.
https://doi.org/10.1007/bf01406742
16. Patil & Gupta, 2019
Comparison of HTS, Mannitol, and Combination Therapy. World Neurosurgery.
https://doi.org/10.1016/j.wneu.2019.01.051
17. Su et al., 2020
10% HTS vs 20% Mannitol in Large Infarction ICP. Clinical Neurology and Neurosurgery, 200.
https://doi.org/10.1016/j.clineuro.2020.106359
18. Khasiyev et al., 2024
Safety of 3% HTS Peripheral Bolus. Neurocritical Care.
https://doi.org/10.1007/s12028-024-01941-3
19. Holden et al., 2022
HTS Use in Neurocritical Care: Dosing, Safety, Administration. AJHP.
https://doi.org/10.1093/ajhp/zxac368
20. Kolsen-Petersen, 2020
Osmotherapy chapter in Management of Severe TBI.
https://doi.org/10.1007/978-3-030-39383-0_61
Sodium & Osmolality Cutoff References
21. Fink, 2012
Osmotherapy: Mannitol vs HTS. Continuum, 18:640–654.
https://doi.org/10.1212/01.con.0000415432.84147.1e
22. Barkas et al., 2023
Hyponatremia Management in Stroke. Ther Adv Endocrinol Metab.
https://doi.org/10.1177/20420188231163806
23. Shao et al., 2015
HTS for Brain Relaxation & ICP: Meta-analysis. PLOS ONE.
https://doi.org/10.1371/journal.pone.0117314
24. Park & Ko, 2023
Adverse effects & monitoring in Hyperosmolar Therapy. JKMA.
https://doi.org/10.5124/jkma.2023.66.5.303