
How NT-proBNP Is Misused in the ED — And How We Can Fix It
A practical, evidence-based guide for emergency & acute care clinicians.

NT-proBNP is one of the most over-ordered yet misinterpreted tests in the ED.
I see it mismanaged almost daily — used as a standalone “rule-in” test, over-trusted when high, and ignored when low.
But here’s the truth we often forget:
NT-proBNP is incredibly good at ruling OUT heart failure — and incredibly bad at ruling it IN.
This mismatch between expectation and reality fuels confusion, overdiagnosis, and unnecessary admissions.
Let’s break down what NT-proBNP actually tells us, what it cannot tell us, and how to use it correctly in fast-paced emergency care.
—>NT-proBNP: A Reliable Rule-Out Tool
NT-proBNP is most powerful when it is low.
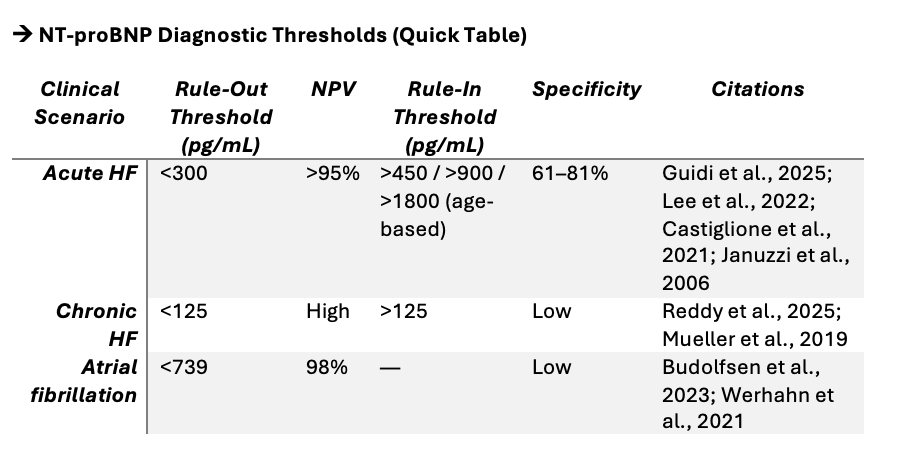
Acute HF excluded: NT-proBNP <300 pg/mL
Chronic HF excluded: NT-proBNP <125 pg/mL
At these levels, negative predictive values consistently exceed 95%
(Guidi et al., 2025; Lee et al., 2022; Mueller et al., 2019; Castiglione et al., 2021; Januzzi et al., 2006).
In the ED, a low NT-proBNP is your friend:
fast reassurance, faster decisions, and fewer unnecessary admissions.
—>Why NT-proBNP Fails as a Rule-In Test
An elevated NT-proBNP does not mean heart failure.
And that’s where misuse happens most often.
NT-proBNP rises in multiple conditions:
Atrial fibrillation
Renal dysfunction
Old age
Sepsis
Pulmonary hypertension
Anemia
Acute coronary syndrome
Pulmonary embolism
So a high NT-proBNP tells us the heart is stressed, not why.
This is why major guidelines clearly state:
NT-proBNP should never be used alone to diagnose heart failure.
(Mueller et al., 2019; Teleanu et al., 2025; Lee et al., 2022)
A high level should trigger further evaluation, not close the case.
How to Interpret NT-proBNP correctly in the ED
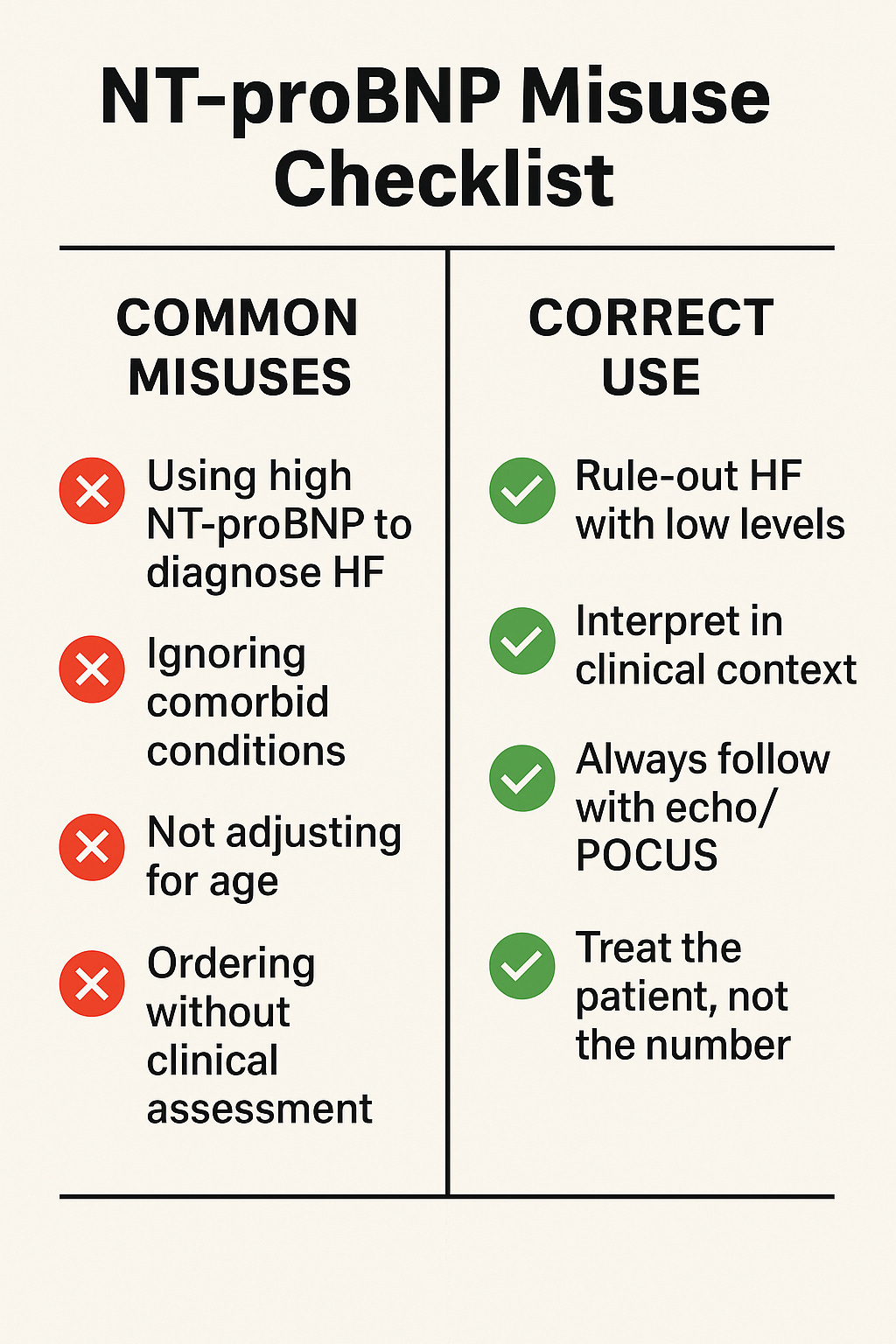
1. Use it early — but only to rule out.
If the level is low, move on confidently.
2. If elevated, interpret with context.
Consider age, rhythm (AF), kidney function, sepsis, and preload status.
3. Never label someone with HF based on NT-proBNP alone.
High values = look deeper, not assume.
4. Always follow up with imaging if uncertain.
Echocardiography remains the confirmation step.
(Mueller et al., 2019; Bayés-Genís et al., 2023)
5. Pair NT-proBNP with clinical assessment — not instead of it.
In Summary
🔹 Low NT-proBNP rules out HF — reliably.
🔹 High NT-proBNP cannot rule in HF — ever.
🔹 Interpretation must consider age, renal function, arrhythmias, and sepsis.
🔹 Always confirm suspected HF with imaging and clinical assessment.
🔹 Misusing NT-proBNP leads to overdiagnosis and unnecessary admissions.
This is a simple test, but it requires thoughtful use.
Let’s stop expecting NT-proBNP to answer questions it was never designed to answer.
References
Guidi, J., Allen, B., Headden, G., Winden, N., Alahapperuma, D., Christenson, R., Peacock, W., & Januzzi, J. (2025). A novel NT-proBNP assay for heart failure diagnosis: A prospective, multicenter clinical trial. Clinica Chimica Acta, 120249. https://doi.org/10.1016/j.cca.2025.120249
Bayés-Genís, A., Doherty, K., Petrie, M., Januzzi, J., Mueller, C., Andreson, L., Bozkurt, B., Butler, J., Chioncel, O., Cleland, J., Christodorescu, R., Del Prato, S., Gustafsson, F., Lam, C., Moura, B., Pop-Busui, R., Seferović, P., Volterrani, M., Vaduganathan, M., Metra, M., & Rosano, G. (2023). Practical algorithms for early diagnosis of heart failure using NT-proBNP. European Journal of Heart Failure, 25. https://doi.org/10.1002/ejhf.3036
Reddy, M., Tada, M., Obokata, M., Carter, P., Kaye, M., Handoko, P., Andersen, P., Sharma, P., Tedford, M., Redfield, M., & Borlaug, M. (2025). Evidence-Based Application of Natriuretic Peptides in Chronic HFpEF. Circulation, 151, 976–989. https://doi.org/10.1161/circulationaha.124.072156
Budolfsen, C., Schmidt, A., Lauridsen, K., Hoeks, C., Waziri, F., Poulsen, C., Riis, D., Rickers, H., & Løfgren, B. (2023). NT-proBNP cut-off for ruling out HF in AF — a prospective study. American Journal of Emergency Medicine, 71, 18–24. https://doi.org/10.1016/j.ajem.2023.05.041
Lee, K., Doudesis, D., Anwar, M., Astengo, F., Chenevier-Gobeaux, C., Claessens, Y., Wussler, D., Kozhuharov, N., Strebel, I., Sabti, Z., deFilippi, C., Seliger, S., … Lindsell, C. (2022). Decision support tool for acute HF diagnosis. BMJ, 377. https://doi.org/10.1136/bmj-2021-068424
Mueller, C., McDonald, K., De Boer, R., Maisel, A., Cleland, J., Kozhuharov, N., Coats, A., Metra, M., Mebazaa, A., Ruschitzka, F., … Januzzi, J. (2019). HFA-ESC practical guidance on natriuretic peptide use. European Journal of Heart Failure, 21. https://doi.org/10.1002/ejhf.1494
Teleanu, I., Mîrșu-Păun, A., Bejan, C., & Stănescu, A. (2025). NT-proBNP for HF screening in primary care. Epidemiologia, 6. https://doi.org/10.3390/epidemiologia6010002
Januzzi, J., Van Kimmenade, R., Lainchbury, J., Bayés-Genís, A., Ordóñez-Llanos, J., Santalo-Bel, M., Pinto, Y., & Richards, M. (2006). NT-proBNP for diagnosis and short-term prognosis in acute HF. European Heart Journal, 27, 330–337. https://doi.org/10.1093/eurheartj/ehi631
Ontario Health Technology Assessment Series (2021). Use of BNP and NT-proBNP as diagnostic tests. 21(2), 1–125.
Werhahn, S., Becker, C., Mende, M., Haarmann, H., Nolte, K., Laufs, U., Zeynalova, S., Löffler, M., Dagres, N., Husser, D., … Wachter, R. (2021). NT-proBNP as a marker for AF and HF. ESC Heart Failure, 9, 100–109. https://doi.org/10.1002/ehf2.13703
Castiglione, V., Aimo, A., Vergaro, G., Saccaro, L., Passino, C., & Emdin, M. (2021). Biomarkers for HF diagnosis and management. Heart Failure Reviews, 27, 625–643. https://doi.org/10.1007/s10741-021-10105-w
Riccardi, M., & Pagnesi, M. (2024). Refining acute HF diagnosis in the elderly. ESC Heart Failure, 11, 3463–3465. https://doi.org/10.1002/ehf2.15017