
Heat-Related Illnesses
Recognition, Rapid Cooling & Evidence-Based Management and Prevention

By-
Dr Arihant Jain, MD | lifeonthefrontline.com
Instagram: @humans.of.em
X - dr__hunt
—————————————————————————
Every summer shift now feels different.
More elderly patients arriving confused during heat waves.
Construction workers collapsing at worksites.
Young athletes becoming encephalopathic after training sessions.
Children arriving lethargic after being left briefly inside vehicles.
Heat-related illness is no longer an uncommon seasonal presentation. It is becoming a daily emergency medicine problem worldwide.
And the dangerous part is this:
Heat stroke is one of the few critical illnesses where definitive treatment begins before the diagnosis is fully confirmed.
If the patient is hot, altered, and crashing:
Cooling is a part of Resuscitation.
Heat Illness Is a Spectrum
Heat-related illness exists on a continuum ranging from minor self-limited conditions to catastrophic multiorgan failure (Gauer & Meyers, 2019).
The spectrum includes:
Heat rash
Heat edema
Heat cramps
Heat syncope
Heat exhaustion
Heat stroke
Most patients initially present somewhere in the middle of this spectrum. Missing progression is what kills.
The Physiology: Why the Body Fails
The human body normally dissipates heat through:
Evaporation
Radiation
Convection
Conduction
As ambient temperatures and humidity rise, these mechanisms become progressively ineffective (CorePendium, 2025).
Once environmental temperature approaches body temperature:
Sweat evaporation becomes inadequate
Peripheral vasodilation worsens hypotension
Cardiac output becomes strained
Splanchnic perfusion decreases
Cellular proteins begin to denature
Cytokine-mediated inflammation escalates
Heat stroke rapidly evolves into a systemic inflammatory syndrome resembling severe sepsis (Bein, 2023).
This is not simply “fever.”
It is:
Cellular injury
Endothelial dysfunction
Coagulopathy
Organ ischemia
Metabolic collapse
The Most Important Clinical Distinction
Heat Exhaustion vs Heat Stroke
This distinction matters enormously.
Heat Exhaustion
Patients may present with:
Weakness
Heavy sweating
Nausea
Tachycardia
Dizziness
Syncope
Muscle cramps
Core temperature is usually:
<40°C
Mental status remains largely preserved.
Thermoregulation still functions (Wexler, 2002).
Heat Stroke
Heat stroke is defined by:
Core temperature ≥40°C (104* F)
CNS dysfunction
(CorePendium, 2025).
Central nervous system dysfunction is the hallmark.
This may include:
Irritability
Ataxia
Delirium
Confusion
Seizures
Coma
Once CNS dysfunction appears in the setting of hyperthermia:
Assume heat stroke until proven otherwise.
Because waiting delays cooling.
And delayed cooling worsens mortality (Sorensen & Hess, 2022).
Exertional vs Classic Heat Stroke: Same Endpoint, Different Patient
One of the most clinically important distinctions in heat-related illness is understanding the difference between Exertional Heat Stroke (EHS) and Classic/Non-exertional Heat Stroke (CHS/NEHS).
While both share the same final pathway — severe hyperthermia, systemic inflammation, coagulopathy, and multiorgan dysfunction — the triggers, patient populations, and clinical patterns differ significantly (Bouchama et al., 2022; Leon & Bouchama, 2015).
Exertional Heat Stroke (EHS)
EHS typically occurs in:
Athletes
Military recruits
Outdoor laborers
Young healthy individuals performing intense physical activity
The mechanism is:
Excess endogenous heat production overwhelming the body’s heat dissipation capacity.
Importantly, EHS can occur even in temperate climates when exercise intensity exceeds heat loss capacity (Garcia et al., 2022; Périard et al., 2022).
Clinically, EHS patients often:
Continue sweating
Develop profound rhabdomyolysis
Have severe metabolic acidosis
Show higher rates of acute kidney injury
Despite appearing critically ill, outcomes are often excellent if cooling is initiated rapidly. Mortality is substantially lower compared with classic heat stroke when evidence-based cooling protocols are followed (Bouchama et al., 2022).
This is why sports medicine and military protocols emphasize:
“Cool first, transport second.”
Cold-water immersion initiated directly in the field dramatically improves neurologic outcomes and survival (Roberts et al., 2023; Belval et al., 2018).
Classic / Non-exertional Heat Stroke (CHS)
Classic heat stroke typically affects:
Elderly individuals
Infants and young children
Patients with chronic illness
Socially isolated individuals
Patients during prolonged heat waves
The trigger is usually:
Passive environmental heat exposure combined with impaired thermoregulation.
(Bouchama et al., 2022; Bukhari, 2023).
These patients often present later, are physiologically fragile, and may have:
Altered mental status
Hot dry skin
Cardiovascular collapse
Delayed recognition
Classic heat stroke carries substantially higher mortality, reaching nearly 60% in some reports (Bouchama et al., 2022).
Unlike EHS, where collapse during exercise immediately raises concern, classic heat stroke is frequently mistaken for:
Sepsis
Stroke
Toxicologic emergencies
Delirium
CNS infection
This diagnostic delay contributes significantly to poor outcomes.
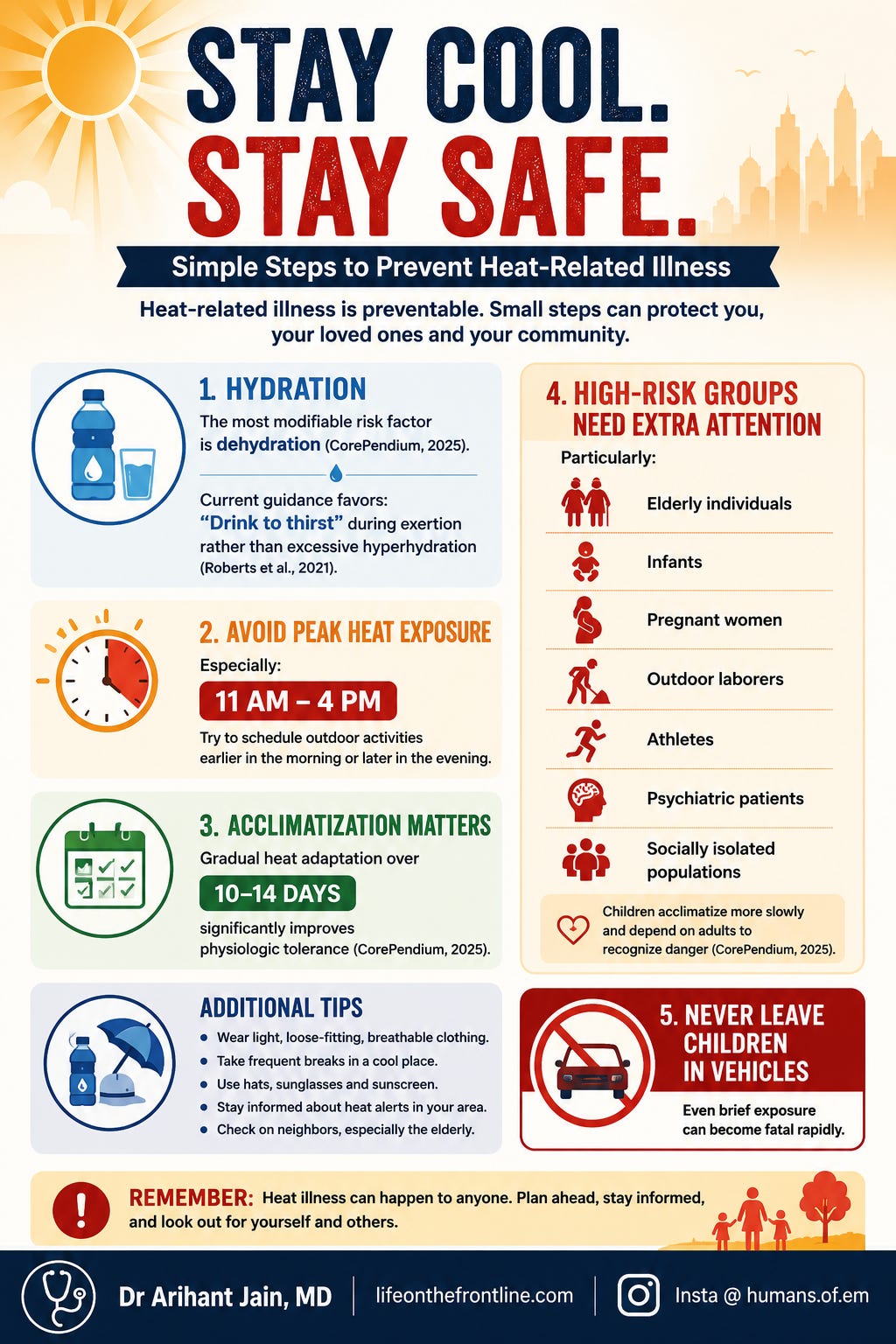
The Patients We Commonly Miss
Heat stroke is not limited to athletes.
Classic heat stroke often affects:
Elderly patients
Socially isolated individuals
Psychiatric patients
Patients without access to cooling
Individuals on anticholinergics, neuroleptics, or sympathomimetics
(CorePendium, 2025).
Exertional heat stroke affects:
Athletes
Military personnel
Outdoor workers
Laborers using heavy protective equipment
Importantly:
Exertional heat stroke can occur even in temperate climates (Roberts et al., 2021).
The ED Approach: Think Fast, Cool Faster
1. Airway & Breathing
Airway management follows standard indications.
But there is an important nuance:
Some patients improve dramatically after cooling.
CorePendium (2025) notes that temporary oxygenation and ventilatory support may bridge patients while rapid cooling is initiated.
If intubation is required:
Rocuronium is preferred
Benzodiazepines are useful for seizure control and sedation
2. Circulation
These patients are profoundly volume depleted.
Start with:
1–2 L isotonic crystalloids
Frequent reassessment
(CorePendium, 2025).
But remember:
Not all hypotension is dehydration alone.
Peripheral vasodilation, systemic inflammation, and myocardial injury all contribute to shock physiology.
Myocardial injury occurs in up to 21% of patients and may precipitate arrhythmias or cardiac arrest (CorePendium, 2025).
Cooling Is the Definitive Treatment
Not antibiotics.
Not vasopressors.
Not antipyretics.
Cooling.
Rapid cooling is the single most important intervention in heat stroke (Barletta et al., 2025).
And critically:
Cooling should begin immediately — even before the full workup is complete.
(CorePendium, 2025).
Cold Water Immersion: The Gold Standard
Among all cooling modalities:
Cold water immersion remains the fastest and most effective.
Preferred water temperature:
1–17°C
Evidence consistently demonstrates:
Faster core temperature reduction
Better neurologic outcomes
Lower mortality
This is especially true in exertional heat stroke (Douma et al., 2020; Pryor et al., 2015).
Modern ED adaptations include:
Ice-water body bags
Portable immersion setups
Athletic event cooling stations
The old concern regarding shivering and peripheral vasoconstriction should not delay immersion therapy. Benefits far outweigh risks (CorePendium, 2025).
If Immersion Is Not Possible
Evaporative cooling remains an effective alternative.
Technique:
Remove clothing
Spray tepid water
Apply high-flow fans
(CorePendium, 2025).
Additional adjuncts:
Ice sheets
Rotating ice towels
Whole-body ice packs
Cooling blankets
Cold IV fluids
But cold IV fluids alone are insufficient (Smith, 2005).
A Common Pitfall: Waiting for “True” Hyperthermia
One of the most dangerous delays occurs when clinicians wait for temperatures above 40°C before initiating cooling.
In altered hyperthermic patients, cooling should not be delayed even if the measured temperature is below 40°C.
Why?
Because:
Temperatures continue rising
Prehospital cooling may transiently reduce readings
Delay worsens organ injury
Clinical suspicion matters more than exact numbers.
What Should NOT Be Used
Antipyretics:
Paracetamol
NSAIDs
have no role.
Dantrolene also lacks evidence of benefit (Barletta et al., 2025).
Heat stroke is not a hypothalamic set-point problem like infectious fever.
Using antipyretics may actually worsen hepatic and renal injury (Glazer, 2005).
The Organ Damage We Must Anticipate
Heat stroke is a multiorgan disease.
Clinicians should actively monitor for:
Rhabdomyolysis
Hyperkalemia
Acute kidney injury
Liver injury
DIC
ARDS
Cardiac dysrhythmias
CK >5,000 U/L suggests significant muscle injury.
CK >16,000 U/L correlates with higher renal failure risk (CorePendium, 2025).
AST >1000 is associated with mortality (CorePendium, 2025).
Importantly:
Coagulopathy often worsens over 24–72 hours, meaning initially stable patients can deteriorate later (Savioli et al., 2022).
Disposition: Do Not Underestimate Heat Stroke
Most minor heat illnesses can safely be discharged after observation and symptom improvement.
But:
All heat stroke patients require admission.
Usually ICU admission.
(CorePendium, 2025).
Why?
Because end-organ injury may evolve hours after initial stabilization.
Prevention: The Most Effective Treatment
Heat illness is largely preventable.
Final Thoughts
Heat-related emergencies are increasing worldwide.
For clinicians, the priorities are remarkably simple:
Recognize early
Measure core temperature
Cool aggressively
Anticipate organ failure
Monitor beyond apparent recovery
Because in heat stroke:
Time to cooling determines outcome.
And often:
Cooling itself is the lifesaving intervention.
References
Adapted from CorePendium chapter on Heat Related Emergencies by Cindy Bitter and team.
Barletta J et al. (2024). Management of Heat-Related Illness and Injury in the ICU. Critical Care Medicine.
Barletta J et al. (2025). SCCM Guidelines for the Treatment of Heat Stroke. Critical Care Medicine.
Bein T. (2023). Pathophysiology and management of heat illness.
Douma M et al. (2020). Cooling techniques for heat stroke. Resuscitation.
Gauer R & Meyers B. (2019). Heat-Related Illnesses. American Family Physician.
Glazer J. (2005). Management of heatstroke and heat exhaustion.
Pryor R et al. (2015). Exertional Heat Illness. Prehospital and Disaster Medicine.
Roberts W et al. (2021). ACSM Consensus on Exertional Heat Illness. Current Sports Medicine Reports.
Savioli G et al. (2022). Heat-Related Illness in Emergency and Critical Care. Biomedicines.
Smith J. (2005). Cooling methods used in exertional heat illness.
Sorensen C & Hess J. (2022). Treatment and Prevention of Heat-Related Illness. NEJM.