
End-Tidal CO₂ (ETCO₂): What the Evidence Actually Supports?
ETCO₂ is one of the most versatile monitors in emergency medicine—but only if we use it for what it truly reflects.

Capnography has become ubiquitous in modern EDs: on monitors, ventilators, transport stretchers, and sedation carts. Yet despite widespread use, ETCO₂ is frequently misinterpreted as a simple ventilation number, which it is not.
This post summarizes where ETCO₂ adds strong, evidence-based value in the ED, where it should be interpreted cautiously, and where it should not be used as a surrogate for arterial CO₂.
What ETCO₂ Physiologically Represents
ETCO₂ reflects the interaction of three physiologic domains:
Ventilation – alveolar ventilation
Perfusion – pulmonary blood flow / cardiac output
Metabolism – CO₂ production
Any disturbance in one domain alters ETCO₂.
This is precisely why ETCO₂ is powerful in emergency care—and why it is dangerous when interpreted in isolation.
Evidence-Based Uses of ETCO₂ in the ED
1. Airway Confirmation and Continuous Airway Monitoring
Highest level of clinical consensus.
Continuous adequate waveform capnography is the most specific method for confirming tracheal intubation, even in transport settings.
No or bad waveform on monitors doesn’t confirm anything, like in arrest scenario.
Loss of ETCO₂ waveform reliably identifies:
Esophageal intubation
Tube displacement
Circuit disconnection
Evidence
Donald & Paterson, EMJ, 2006
Long et al., J Emerg Med, 2017
Sandroni et al., Resuscitation, 2018
➡️ In the ED, ETCO₂ is mandatory for airway safety, not optional.
2. Cardiac Arrest and CPR Quality
During CPR, ETCO₂ primarily reflects pulmonary blood flow, making it a real-time surrogate of cardiac output.
Key evidence-based roles:
ETCO₂ <10 mmHg → poor CPR quality / poor prognosis
Rising ETCO₂ → improving chest compressions
Sudden increase in ETCO₂ → ROSC until proven otherwise
Evidence
Sandroni et al., Resuscitation, 2018
Long et al., J Emerg Med, 2017
No other bedside monitor provides such immediate feedback during resuscitation.
3. Shock and Undifferentiated Hypotension
In shock states, ETCO₂ correlates more strongly with perfusion than ventilation.
Low ETCO₂ is associated with:
High lactate
Low MAP and cardiac output
Increased mortality
Prospective ED studies demonstrate that ETCO₂ on arrival predicts in-hospital mortality in non-traumatic shock.
Evidence
Kheng & Rahman, Int J Emerg Med, 2012
Ekka et al., Turkish J Emerg Med, 2025
López-Izquierdo et al., AJEM, 2024 & 2025
➡️ In shock, ETCO₂ is best used as a resuscitation trend marker, not a target.
4. Procedural Sedation and Early Detection of Hypoventilation
Multiple ED and peri-procedural studies show that ETCO₂ detects respiratory depression earlier than pulse oximetry.
ETCO₂ rises or waveform loss often precedes:
Desaturation
Clinical apnea
Evidence
Miner et al., Acad Emerg Med, 2002
Burton et al., Acad Emerg Med, 2006
Camacho et al., J PeriAnesthesia Nurs, 2021
This makes ETCO₂ a safety monitor, not merely a respiratory parameter.
5. Metabolic Acidosis and Respiratory Compensation (Adjunct Only)
ETCO₂ correlates modestly with bicarbonate and pH in conditions such as DKA and sepsis, but correlation is population-level, not patient-specific.
Reported correlation coefficients typically range from r ≈ 0.3–0.6
ETCO₂ frequently underestimates PaCO₂ in critically ill patients due to:
Shock
Increased dead space
V/Q mismatch
Evidence
Kartal et al., Am J Emerg Med, 2011
Taghizadieh et al., J Cardiovasc Thorac Res, 2016
Aminiahidashti et al., Emergency (Tehran), 2018
➡️ ETCO₂ can screen for metabolic acidosis, but cannot replace ABG/VBG for ventilatory decisions.
Where the Evidence Warns Against Over-Interpretation
❌ Using ETCO₂ as a PaCO₂ Surrogate in Critical Illness
Large ICU, trauma, and transport studies show:
PaCO₂–ETCO₂ gradient ≥10 mmHg in 40–60% of critically ill patients
Gradient widens unpredictably in shock and lung injury
Evidence
Cooper et al., Prehosp Disaster Med, 2013
Campion et al., J Trauma Acute Care Surg, 2019
Martin-Gill et al., Prehospital Emerg Care, 2024
ETCO₂ should not be used alone to judge adequacy of ventilation in:
Shock
Severe metabolic acidosis
ARDS
Multi-organ failure
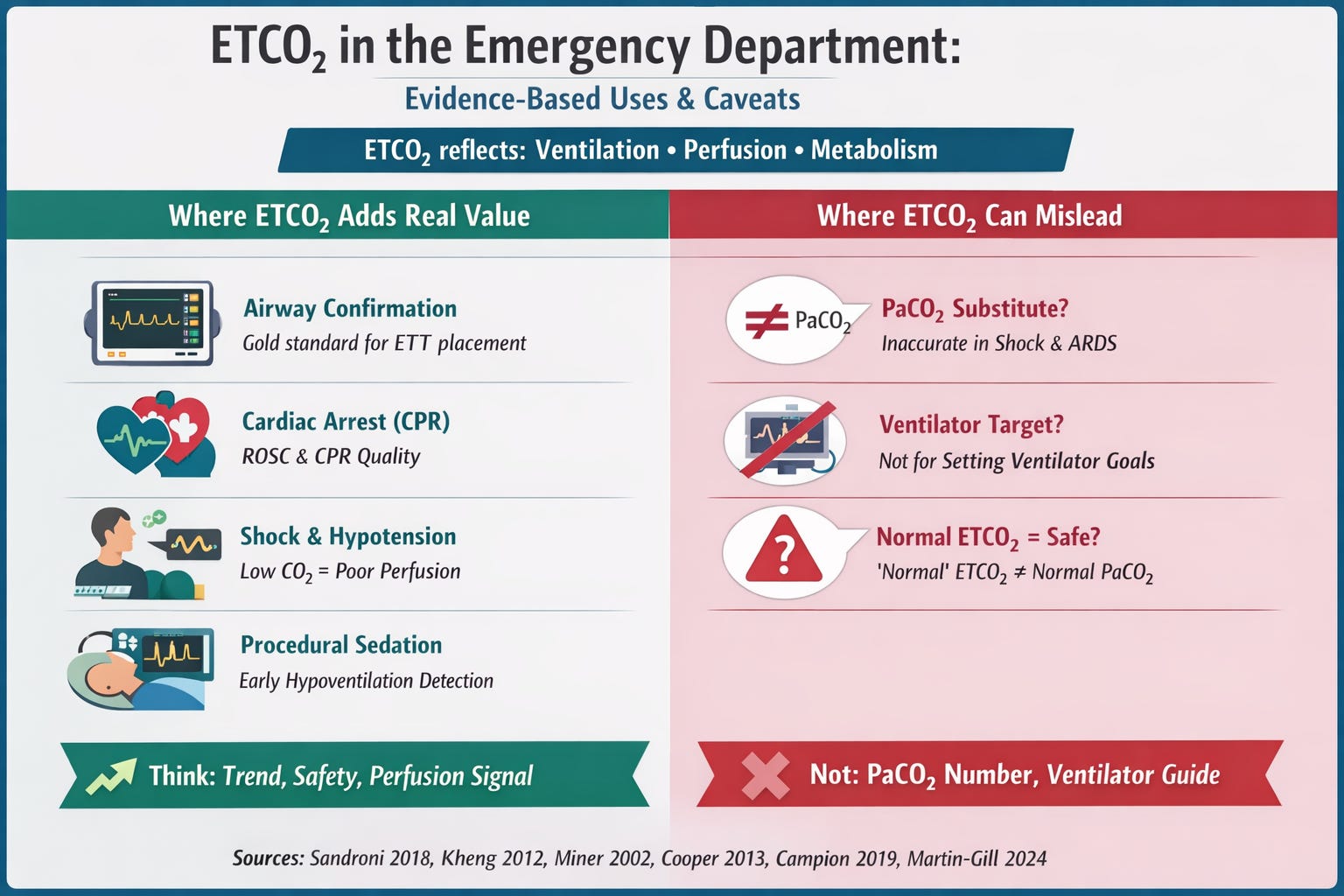
Practical ; Take-Home
Always use ETCO₂ for airway confirmation and CPR
Trust trends, not isolated values
Low ETCO₂ in shock = poor perfusion until proven otherwise
Do not use ETCO₂ alone to guide ventilatory compensation
ABG/VBG remain essential in critically ill patients
In the emergency department, ETCO₂ is most powerful when used as a trend-based, physiology-informed monitor. It saves lives when interpreted in context—and misleads when treated as just another number.
References
Miner JR, Heegaard W, Plummer D. End-tidal carbon dioxide monitoring during procedural sedation. Acad Emerg Med. 2002;9(4):275-280. doi:10.1197/aemj.9.4.275
Burton JH, Harrah JD, Germann CA, Dillon DC. Does end-tidal carbon dioxide monitoring detect respiratory events prior to current sedation monitoring practices? Acad Emerg Med. 2006;13(5):500-504. doi:10.1197/j.aem.2005.12.017
Donald MJ, Paterson B. End tidal carbon dioxide monitoring in prehospital and retrieval medicine: a review. Emerg Med J. 2006;23(9):728-730. doi:10.1136/emj.2006.037184
Long B, Koyfman A, Vivirito MA. Capnography in the emergency department: a review of uses, waveforms, and limitations. J Emerg Med. 2017;53(6):829-842. doi:10.1016/j.jemermed.2017.08.026
Sandroni C, De Santis P, D’Arrigo S. Capnography during cardiac arrest. Resuscitation. 2018;132:73-77. doi:10.1016/j.resuscitation.2018.08.018
Kheng CP, Rahman NH. The use of end-tidal carbon dioxide monitoring in patients with hypotension in the emergency department. Int J Emerg Med. 2012;5:31. doi:10.1186/1865-1380-5-31
Ekka M, Sreekumar A, Aggarwal P, et al. Utility of end-tidal carbon dioxide monitoring in predicting in-hospital mortality in nontraumatic shock in the emergency department. Turk J Emerg Med. 2025;25(3):199-207. doi:10.4103/tjem.tjem_223_24
López-Izquierdo R, Martín-Rodríguez F, Sanz-García A, et al. Utility of noninvasive capnography and perfusion index in adult emergency department patients. Am J Emerg Med. 2024;79:85-90. doi:10.1016/j.ajem.2024.02.017
López-Izquierdo R, Martín-Rodríguez F, Cuadrillero R, et al. National Early Warning Score 2 plus capnography and perfusion index to estimate poor outcomes in emergency departments. Am J Emerg Med. 2025;90:16-22. doi:10.1016/j.ajem.2025.01.011
Kartal M, Eray O, Rinnert S, et al. ETCO₂: a predictive tool for excluding metabolic acidosis in emergency department patients. Am J Emerg Med. 2011;29(1):65-69. doi:10.1016/j.ajem.2009.01.018
Taghizadieh A, Pouraghaei M, Moharamzadeh P, et al. Correlation between end-tidal CO₂ and arterial blood gas parameters in patients with metabolic acidosis. J Cardiovasc Thorac Res. 2016;8(3):98-101. doi:10.15171/jcvtr.2016.19
Aminiahidashti H, Shafiee S, Kiasari AZ, Sazgar M. Applications of end-tidal carbon dioxide monitoring in emergency department; a narrative review. Emergency (Tehran). 2018;6(1):e5.
Cooper CJ, Kraatz JJ, Kubiak DW, et al. The relationship between end-tidal CO₂ and arterial CO₂ in critically ill trauma patients. Prehosp Disaster Med. 2013;28(1):87-93. doi:10.1017/S1049023X1200164X
Campion EM, Peltan ID, Brown SM, et al. Discordance between end-tidal and arterial carbon dioxide measurements in critically ill patients. J Trauma Acute Care Surg. 2019;87(5):1038-1045. doi:10.1097/TA.0000000000002465
Martin-Gill C, Guyette FX, Rittenberger JC, et al. Accuracy of end-tidal carbon dioxide in critically ill and injured patients during transport. Prehosp Emerg Care. 2024;28(1):1-9. doi:10.1080/10903127.2023.2243127