
Dizzy: No more !
The approach to giddiness: thinking in syndromes, not symptoms

“Giddiness” is one of those ED complaints that feels deceptively benign—yet quietly carries the risk of missed posterior circulation stroke. Acute dizziness accounts for roughly 3–4% of ED visits, with nearly 1 in 5 patients admitted. Stroke remains uncommon, but consistently over-investigated with CT and under-diagnosed clinically.
The modern, evidence-based shift—crystallised in GRACE-3—is simple but profound: stop chasing symptom quality (“vertigo vs presyncope”) and start thinking in timing, triggers, eye movements, gait, and red flags (Edlow et al., 2023).
This post walks through a bedside-first, syndrome-based approach you can use on your next dizzy patient—without defaulting to CT or medications.
Before we start: what do patients mean by “giddiness”?
Before diving into algorithms, eye movements, and imaging decisions, it’s worth addressing the word that brings many patients to the ED in the first place: “giddiness.” In clinical practice, patients use dizzy, giddy, woozy, light-headed, off-balance, or spinning interchangeably—and often change their description within the same conversation (Sloane et al., 2001; Broomfield et al., 2008; Sommerfeldt et al., 2020).
Research consistently shows that these labels overlap heavily and have poor diagnostic reliability, which is why modern guidelines advise clinicians not to anchor on the word itself but instead focus on timing, triggers, associated symptoms, eye movements, and gait (Edlow et al., 2018; Gurley & Edlow, 2019; Muncie et al., 2017).
In many ENT and clinical literature, “giddiness” is simply used as a broad umbrella term for dizziness or vertigo rather than a distinct entity (Ranjan et al., 2020; Ramchandra, 2021; Thomas et al., 2018). With that context, the section below clarifies how these terms are used—and why, in the ED, the word matters far less than the bedside exam that follows.
Why “giddiness” is hard in the ED
Dizzy patients are heterogeneous, time-consuming, and cognitively taxing. About 10% have a neurological cause, and one-third of those are cerebrovascular (Edlow et al., 2023; Nouini et al., 2023).
Traditional teaching tried to subtype dizziness by patient-described quality—vertigo, presyncope, disequilibrium, light-headedness. Multiple studies now show this performs poorly and often misleads clinicians (Edlow et al., 2023; Tarnutzer et al., 2025).
GRACE-3 reframes dizziness as a single symptom and recommends classification by:
Timing
Triggers
Associated signs (especially eye movements and gait)
Think of eye movements and gait as vital signs of the posterior fossa.
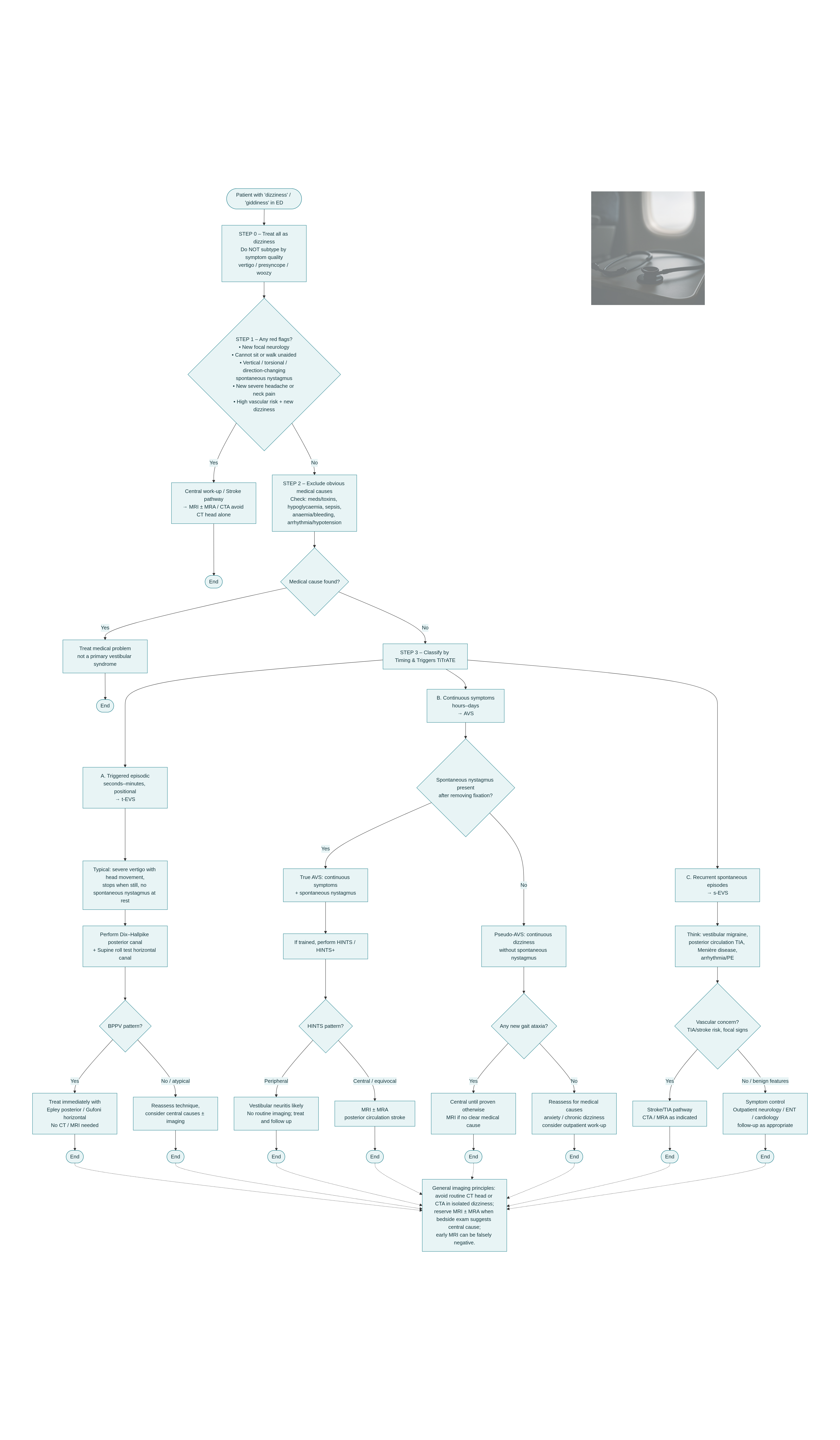
Step 1: Frame the presentation (TiTrATE) + red flags
Use the TiTrATE approach to classify dizziness into one of three syndromes (Edlow et al., 2023; Stewart et al., 2022; Tarnutzer et al., 2025):
Triggered episodic (seconds–minutes, positional)
Acute vestibular syndrome (AVS) (continuous ≥24 h)
Spontaneous episodic (recurrent, untriggered)
At the same time, screen aggressively for red flags:
New focal neurological deficits
Severe gait or truncal ataxia
New headache or neck pain (consider vertebral dissection)
Multiple vascular risk factors
Inability to sit or stand independently
Roughly one-third of neurological dizziness is cerebrovascular, so this screen matters (Edlow et al., 2023; Gerlier et al., 2025; Ota et al., 2023).
Step 2: Exclude obvious medical causes
Up to half of dizzy ED patients have systemic causes:
Drug toxicity
Hypovolaemia/anaemia
Sepsis
Arrhythmia
Metabolic derangements - like hypoglycaemia, dehydration, etc.
A focused history, vitals, ECG, glucose, and targeted labs often identify this group (Ota et al., 2023; Nouini et al., 2023).
If a clear medical diagnosis explains symptoms and no neurological red flags or concerning ataxia are present, manage the medical problem and reassess.
Step 3: Recognise the vestibular syndrome
a). Triggered episodic vestibular syndrome (t-EVS)
This is the most common vestibular pattern in the ED.
Key features
Brief episodes (seconds–minutes)
Clearly triggered by head position
Severe symptoms stop completely when still
Think BPPV first.
Bedside diagnosis
Dix–Hallpike → posterior canal BPPV
Supine roll test → horizontal canal BPPV
Treatment
Treat immediately with canalith repositioning (Epley/Gufoni)
This reduces imaging, ED length of stay, and revisits (Edlow & Kerber, 2022; Gerlier et al., 2025; Stewart et al., 2022)
—> Typical BPPV needs no CT or MRI.
b). Acute vestibular syndrome (AVS)
AVS = continuous dizziness/vertigo, nausea, postural instability, usually with spontaneous nystagmus.
Two clinically important subgroups:
True AVS: continuous symptoms with spontaneous nystagmus
Pseudo-AVS: continuous dizziness without spontaneous nystagmus
True AVS (only indication for HINTS )
If trained, perform HINTS/HINTS+
Peripheral pattern → vestibular neuritis likely
Central or equivocal → MRI >>> CT
HINTS+ outperforms early MRI in the first 24–48 h when used correctly (Edlow et al., 2023; Tarnutzer et al., 2025)
Pseudo-AVS
HINTS is not validated
Any new gait ataxia is concerning
Central causes must be excluded unless a clear medical explanation exists
Imaging pearl
Early MRI can be false-negative in up to 20% within 24–48 h
Use imaging as confirmation, not replacement, for bedside assessment (Edlow et al., 2023).
A critical note on HINTS: powerful, but only in the right hands and the right patients
Because HINTS is often described as being “more sensitive than MRI,” it has acquired an almost mythic status in emergency medicine. That reputation, however, only holds within a very narrow clinical niche. The evidence is remarkably consistent: HINTS is highly accurate only when applied to patients with true acute vestibular syndrome (AVS) and when performed by clinicians trained in neuro-otologic examination (Kattah, 2018; Ohle et al., 2020; Gottlieb et al., 2022).
In practice, this nuance is frequently lost. Multiple ED studies show that HINTS is commonly performed in patients without continuous symptoms, without spontaneous nystagmus, or with positional dizziness, where it was never intended to be used. In these populations, its diagnostic performance collapses, creating false reassurance or unnecessary alarm (Dmitriew et al., 2020; Nolan et al., 2025; Akhter et al., 2023).
When is HINTS actually useful?
HINTS should be reserved for a very specific clinical phenotype:
Continuous dizziness/vertigo lasting hours to days
Spontaneous nystagmus present at rest (after removing fixation)
Gait unsteadiness
No obvious alternative explanation such as intoxication, hypoglycaemia, or sepsis
This is the classic acute vestibular syndrome (AVS) population in which HINTS was derived and validated (Kattah, 2018; Gerlier et al., 2021; Loureiro et al., 2021).
ED data are sobering:
In one large retrospective cohort, 96.9% of HINTS exams were performed in patients who did not meet AVS criteria, rendering the test essentially useless (Dmitriew et al., 2020).
Other studies show ~70% inappropriate use, most commonly in patients without nystagmus, a group in whom HINTS has no evidentiary basis (Nolan et al., 2025; Akhter et al., 2023).
Using HINTS outside AVS blurs it with Dix–Hallpike populations, inflates false positives, and undermines its credibility altogether (Kattah, 2019; Loureiro et al., 2021).
What this means for ED practice?
Population matters more than the test itself: HINTS is not a “dizziness exam”; it is an AVS exam with spontaneous nystagmus.
Training is non-negotiable: surveys consistently show most frontline clinicians feel under-trained and lack confidence in interpreting eye movements (Warner et al., 2021; Nakatsuka & Molloy, 2022; Rehman et al., 2025).
HINTS does not replace imaging outside its niche: transient symptoms, episodic dizziness, nystagmus-negative patients, or untrained examiners should prompt alternative pathways, often including MRI when central disease is a concern (Srinivasan & Tirschwell, 2023; Tarnutzer & Edlow, 2023).
This video by Dr Peter - shows correct way to perform it.
c). Spontaneous episodic vestibular syndrome (s-EVS)
Recurrent, untriggered episodes of dizziness/vertigo.
Key differentials
Vestibular migraine
Posterior circulation TIA
Menière disease
Episodic arrhythmia or PE
If vascular concern exists, pursue CTA/MRA, not non-contrast CT, and manage via stroke/TIA pathways (Vanni et al., 2024; Kozlowski et al., 2025).
Sudbury Vertigo Risk Score - some insights
The Sudbury Vertigo Risk Score (SVRS) is a 7-item bedside clinical tool designed for emergency departments to estimate the risk that dizziness or vertigo is due to a serious central cause such as stroke, TIA, vertebral artery dissection, or brain tumor (Ohle et al., 2024; Van Patot et al., 2025). It incorporates male sex, age >65, diabetes, hypertension (heavily weighted), focal motor or sensory deficits, cerebellar signs such as ataxia or dysmetria, and a protective deduction for clear benign paroxysmal positional vertigo (BPPV) (Ohle et al., 2024). In derivation and validation cohorts including more than 6,000 patients, the SVRS demonstrated excellent discriminatory performance (C-statistic ~0.95–0.96), with patients scoring <5 having nearly 0% risk of serious diagnoses and 100% sensitivity, while risk increased substantially with higher scores (Ohle et al., 2024; Van Patot et al., 2025).
How to use it: The SVRS should be calculated after a focused history and thorough neurological examination. Patients with scores <5 may be considered low risk and potentially discharged without advanced imaging if clinically stable, whereas scores ≥5 should prompt further investigation with neuroimaging and/or neurology consultation based on the overall clinical picture (Ohle et al., 2024).
When to use it: It is most useful in adult ED patients presenting with dizziness, vertigo, or imbalance when differentiating peripheral from possible central causes is uncertain (Van Patot et al., 2025).
When not to use it: The score should not replace clinical judgment and should not be applied in patients with clear stroke syndromes, unstable vital signs, altered mental status, or when a reliable neurological exam cannot be performed. Concerns have also been raised about diagnostic complexity and overreliance on risk scores alone (Günay et al., 2025).
Take-home message
Giddiness in the ED should no longer trigger reflex CT and meclizine.
Instead, anchor your approach in:
Syndromes (TiTrATE)
Bedside eye movements and gait
Selective, purposeful imaging
Early curative treatment for BPPV
This is how we miss fewer strokes while doing less harm.
“Educational caution: This framework is for education and bedside reasoning and does not replace clinical judgment, formal training, or local stroke pathways.”
References
Edlow JA, Carpenter CR, Akhter M, et al. Guidelines for reasonable and appropriate care in the emergency department 3 (GRACE-3): acute dizziness and vertigo in the emergency department. Acad Emerg Med. 2023;30(4):442-486. doi:10.1111/acem.14728
Edlow JA, Gurley KL, Newman-Toker DE. A new diagnostic approach to the adult patient with acute dizziness. J Emerg Med. 2018;54(4):469-483. doi:10.1016/j.jemermed.2017.12.024
Gurley KL, Edlow JA. Acute dizziness. Semin Neurol. 2019;39(1):27-40. doi:10.1055/s-0038-1676857
Muncie HL Jr, Sirmans SM, James E. Dizziness: approach to evaluation and management. Am Fam Physician. 2017;95(3):154-162.
Sloane PD, Coeytaux RR, Beck RS, Dallara J. Dizziness: state of the science. Ann Intern Med. 2001;134(9 Pt 2):823-832. doi:10.7326/0003-4819-134-9_part_2-200105011-00005
Broomfield S, Bruce I, Malla J, Kay N. The dizzy patient. Clin Otolaryngol. 2008;33(1):1-7. doi:10.1111/j.1749-4486.2008.01737.x
Sommerfeldt JM, Fischer JL, Morrison D, et al. A dizzying complaint: investigating the intended meaning of dizziness among patients and providers. Laryngoscope. 2021;131(1):E85-E91. doi:10.1002/lary.29271
Ranjan A, Jain S, Chaudhari S. A study of clinical profile in patients with vestibular and non-vestibular vertigo. Int J Curr Res Rev. 2020;12:89-92. doi:10.31782/IJCRR.2020.SP75
Ramchandra R. Clinical evaluation of giddiness: our experience. J Med Sci Clin Res. 2021;9(4):16-20. doi:10.18535/jmscr/v9i4.16
Thomas G, John G, John A. Evaluation of giddiness: a peripheral hospital experience. Int J Otorhinolaryngol Head Neck Surg. 2018;4(3):673-676. doi:10.18203/issn.2454-5929.ijohns20181443
Chan Y. Differential diagnosis of dizziness. Curr Opin Otolaryngol Head Neck Surg. 2009;17(3):200-203. doi:10.1097/MOO.0b013e32832b2594
Kim HA, Bisdorff A, Bronstein AM, et al. Hemodynamic orthostatic dizziness/vertigo: diagnostic criteria. J Vestib Res. 2019;29(2-3):45-56. doi:10.3233/VES-190655
Hillson R. Dizziness in diabetes. Pract Diabetes. 2018;35(3):79-82. doi:10.1002/pdi.2158
Woźniak O, Wąsik J, Gryboś K, et al. Dizziness—causes, symptoms, diagnosis and treatment. J Educ Health Sport. 2025;80:60155. doi:10.12775/JEHS.2025.80.60155
Kattah JC. Use of HINTS in the acute vestibular syndrome: an overview. Stroke Vasc Neurol. 2018;3(4):190-196. doi:10.1136/svn-2018-000160
Kattah JC. Update on HINTS Plus, with discussion of pitfalls and pearls. J Neurol Phys Ther. 2019;43(2):91-98. doi:10.1097/NPT.0000000000000274
Ohle R, Montpellier RA, Marchadier V, et al. Can emergency physicians accurately rule out a central cause of vertigo using the HINTS examination? A systematic review and meta-analysis. Acad Emerg Med. 2020;27(9):887-896. doi:10.1111/acem.13960
Gottlieb M, Peksa GD, Carlson JN. Head impulse, nystagmus, and test of skew examination for diagnosing central causes of acute vestibular syndrome. Cochrane Database Syst Rev. 2022;11:CD015089. doi:10.1002/14651858.CD015089
Dmitriew C, Regis A, Bodunde O, et al. Diagnostic accuracy of the HINTS exam in an emergency department: a retrospective chart review. Acad Emerg Med. 2021;28(4):387-393. doi:10.1111/acem.14171
Gerlier C, Hoarau M, Fels A, et al. Differentiating central from peripheral causes of acute vertigo using HINTS, STANDING, and ABCD2. Acad Emerg Med. 2021;28(12):1368-1378. doi:10.1111/acem.14337
Nolan K, Murray N, Lambert E, Liu W, Akhter M. Improper performance of the HINTS exam in emergency physicians is driven by incorrect use of nystagmus. Am J Emerg Med. 2025;94:185-187. doi:10.1016/j.ajem.2025.04.066
Akhter M, Lambert E, Murray N. Inaccurate use of HINTS exam by emergency physicians in patients with dizziness. Ann Emerg Med. 2023;82(4):S142. doi:10.1016/j.annemergmed.2023.08.380
Tarnutzer AA, Edlow JA. Bedside testing in acute vestibular syndrome—evaluating HINTS Plus and beyond. Audiol Res. 2023;13(5):670-685. doi:10.3390/audiolres13050059
Srinivasan V, Tirschwell DL. Give us some GRACE, we can’t take the HINT: there is still a role for imaging in dizzy patients. Acad Emerg Med. 2023;30(6):707-709. doi:10.1111/acem.14779
Loureiro E, Felippe L, Guimarães A, Costa AMC. HINTS protocol and its accuracy to identify posterior circulation stroke: a review. Sao Paulo Med J. 2021;139(1):78-84. doi:10.5327/Z1516-3180.2021.0446
Krishnan K, Bassilious K, Eriksen E, et al. Posterior circulation stroke diagnosis using HINTS in patients with acute vestibular syndrome. Eur Stroke J. 2019;4(3):233-239. doi:10.1177/2396987319843701
Warner C, Bunn L, Koohi N, et al. Clinicians’ perspectives in using HINTS for acute vestibular syndrome: UK experience. Stroke Vasc Neurol. 2022;7(2):172-175. doi:10.1136/svn-2021-001229
Nakatsuka M, Molloy E. The HINTS examination and STANDING algorithm in acute vestibular syndrome: a systematic review. PLoS One. 2022;17(4):e0266252. doi:10.1371/journal.pone.0266252
Rehman S, Ahmed M, Khan K, et al. Emphasizing the clinical impact of the HINTS examination. J R Coll Physicians Edinb. 2025;55(2):156-157. doi:10.1177/14782715251342124
Ohle R, Savage D, Roy D, et al. Development of a clinical risk score to risk stratify for a serious cause of vertigo in patients presenting to the emergency department. Ann Emerg Med. 2024. doi:10.1016/j.annemergmed.2024.06.003
Van Patot E, Roy D, Baraku E, et al. Validation of the Sudbury Vertigo Risk Score to risk stratify for a serious cause of vertigo. Acad Emerg Med. 2025;32:863-873. doi:10.1111/acem.70017
Günay S, Pakkan A, Öztürk A, Komut S. Diagnostic challenges in vertigo: concerns about the Sudbury Vertigo Risk Score. Ann Emerg Med. 2025;85(6):573-574. doi:10.1016/j.annemergmed.2025.01.011
A very nice post. The problem with HINTS or HINTS Plus is that they are often used when they are not indicated and interpreted outside the correct clinical context, which dilutes their sensitivity. You have beautifully highlighted when not to use HINTS, which is extremely important. Recently I came across an excellent vertigo course designed by Peter Johns, a stalwart in this field, along with Scott Weingart - https://emneuro.com/spinclass/