
Bicarbonate: Myths, Misuse & Where It Truly Matters
Bicarbonate is a precision drug — powerful in the right setting, harmful in the wrong one.

Despite being one of the oldest therapies in emergency medicine, sodium bicarbonate remains one of the most misunderstood. Many times, it gets pushed simply because “the pH is low” — but acidemia is more physiology than chemistry, and improving numbers doesn’t always improve the patient’s condition [1,2].
Where Bicarbonate Is NOT Your First Move
Most metabolic acidosis cases in ED:
❌ Pure lactic acidosis from shock
❌ Sepsis without AKI
❌ Respiratory acidosis
❌ “pH <7.2 ⇒ Give bicarb” reflex
In lactic acidosis from hypoxia, bicarbonate does not improve perfusion, may worsen intracellular acidosis, and adds sodium + fluid load [1,3].
Fix shock → perfusion → lactate first.
Not the ABG.
Where Bicarbonate Actually Helps
Use bicarb when acidemia is no longer adaptive — when it starts hindering organs, especially the kidneys and heart.
Most evidence-supported ED indications:
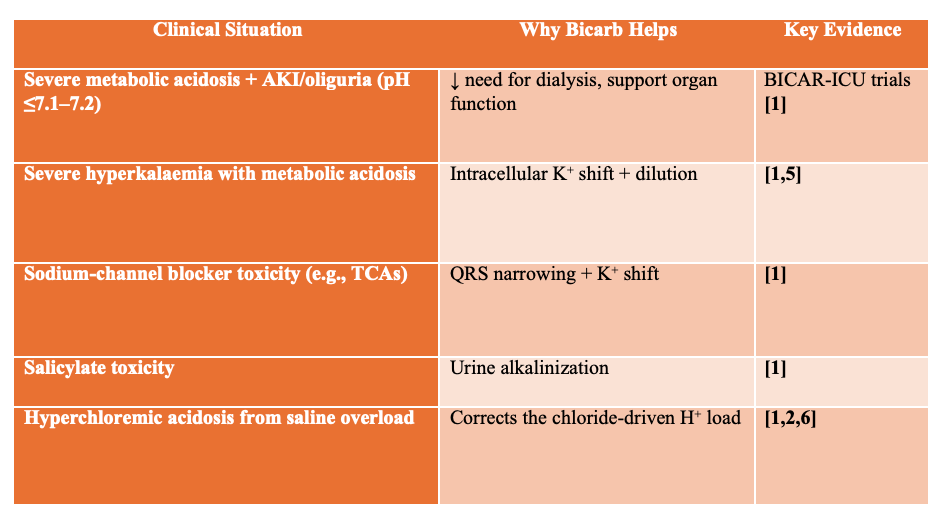
These are targeted, not routine use cases.
Sodium bicarbonate is not a universal antidote to low pH. Its most evidence-supported role is in severe metabolic acidemia with acute kidney injury (AKI) — particularly when pH ≤ 7.1–7.2 and the acidosis is contributing to hemodynamic instability or dialysis risk. The original BICAR-ICU trial (2018) showed reduced KRT requirement and a survival signal in the AKI subgroup, while the more recent BICAR-ICU-2 trial (2025) did not demonstrate mortality benefit overall but did show delayed and reduced KRT use, at the cost of higher sodium load and earlier vasopressor exposure.
Evidence summaries therefore recommend targeted use — not routine buffering — with bicarbonate reserved for patients where organ support and hyperkalemia management are parallel goals. Patients with hyperchloremic acidosis may particularly benefit, as bicarbonate therapy directly reverses chloride-driven acidemia and avoids further saline burden.
Isotonic vs Hypertonic Bicarbonate — Not interchangeable
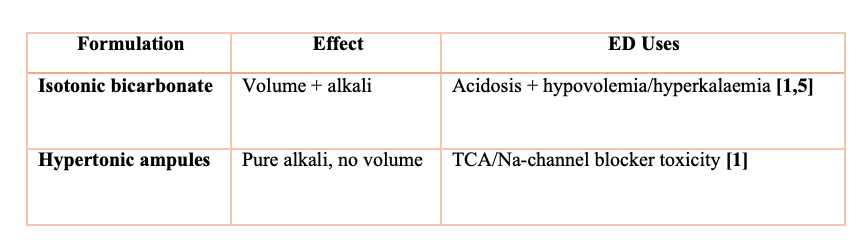
Hypertonic bicarb does not reliably reduce K⁺ due to solute drag [5].
How to Make Isotonic Bicarbonate at the Bedside (ED/ICU Use) [6]
When bicarbonate is indicated as a resuscitation fluid (e.g., hyperkalemia + metabolic acidosis + hypotension), isotonic bicarbonate is preferred over hypertonic boluses. The standard preparation:
Isotonic Bicarbonate Formula:
Add 3 amps of Sodium Bicarbonate (50 mEq each = 150 mEq total)
Into 1 liter of D5W
This results in:
150 mEq/L NaHCO₃ (≈ normal sodium concentration)
Osmolarity ~300 mOsm/L (near-isotonic)
Safe for peripheral IV infusion
Typical ED/ICU infusion rates:
50–150 mL/hr for gradual pH correction
Up to 250 mL/hr in severe metabolic acidosis with shock (close monitoring required)
Key benefits vs hypertonic bicarbonate:
Provides volume + alkali without the osmotic sodium load
Avoids solute drag that can paradoxically raise potassium
Always monitor:
pH, Na⁺, K⁺, Ca²⁺, lactate, and volume status
Repeat blood gases every 2–4 hours
Isotonic bicarbonate = the right tool when volume resuscitation AND acidosis correction are both needed.
Why Undiluted (Hypertonic) Bicarbonate Can Be Harmful in Hyperkalemic Arrest
In cardiac arrest from hyperkalemia, it may be tempting to push undiluted 8.4% sodium bicarbonate (1 mEq/mL) as a rapid fix — but this can worsen serum potassium rather than help. The hypertonic bicarbonate creates a steep extracellular osmotic shift, pulling potassium out of cells and into the bloodstream (“solute drag”), counteracting the desired intracellular driving effect. [5]
Additionally:
Rapid CO₂ generation can worsen intracellular acidosis
Sudden alkalinization can drop ionized calcium, impairing contractility and resuscitation success
Hypernatremia & volume-independent sodium load can worsen neurologic outcomes
Extravasation risk → severe tissue injury
🛑 Hypertonic bicarbonate should not be used as routine push-dose therapy in hyperkalemic arrest.
✔ Best practice during arrest:
IV calcium to stabilize the myocardium
Insulin + dextrose (or beta-agonists) to shift K⁺
Definitive K⁺ removal (dialysis) as soon as feasible
Consider isotonic bicarbonate infusion (not pushes) only if severe metabolic acidosis is present
If you must give bicarbonate in cardiac arrest — know why you are giving it, and ensure the physiology supports it.
What did BICAR-ICU Trials Actually Show?
—> BICAR-ICU [7]
No mortality benefit overall, benefit in AKI subgroup
Use selectively in AKI
—> BICAR-ICU 2 [8]
↓ & delayed dialysis use but ↑ fluid balance + pressors
Organ support > survival
Bicarbonate is not a mortality drug —
it is an organ protection strategy in the right patient.
When Bicarb Can Harm
Situations to avoid or minimize use:
Pure lactic acidosis from early shock [1,3]
Respiratory acidosis (CO₂ retention makes pH worse) [1]
Volume overload (HF, pulmonary edema) [1,2]
Hypernatremia — worsens sodium load [1]
Hypocalcemia — alkalosis ↓ ionized Ca [1]
Hypokalemia [1]
If there is no AKI and no hyperkalemia →
Bicarb is probably not helping.
The Physiology Takeaway
Acidemia is often a protective mechanism.
We intervene only when it becomes maladaptive.
✔️ Better perfusion
✔️ Better potassium handling
✔️ Better organ function
Not:
✘ “prettier ABG”
This is pH-guided resuscitation [6].
Final Take-Home
🩺 Bicarbonate is a precision therapy — not a reflex.
Use it when it meaningfully corrects physiology, avoid when it only adds risk.
Where it helps most
Severe metabolic acidosis with AKI/oliguria
Hyperkalemia with metabolic acidosis (as an adjunct — not primary therapy)
Select toxicology: TCA + sodium-channel blocker toxicity, salicylate poisoning
Significant hyperchloremic acidosis after large-volume NS
Where to avoid
Pure lactic acidosis from hypoperfusion
Respiratory acidosis
Hypernatremia, fluid overload, hypocalcemia
When pH is already >7.2 and patient clinically improving
🚨 Critical Caution
Do NOT push undiluted bicarbonate for hyperkalemia —
it may worsen intracellular acidosis, shift K⁺ out of cells, drop ionized calcium, and delay proven therapies like insulin/dextrose and dialysis.
Think beyond the number (pH) — treat the cause, use bicarbonate only when it changes outcomes.
Buffer the right patient — not the number.
References:-
Kraut JA, Lew SQ, Amlal H, et al. A review of bicarbonate use in common clinical scenarios. J Emerg Med. 2023;64(4):e377–e385.
Semler MW, Self WH, Wanderer JP, et al. Balanced crystalloids versus saline in critically ill adults. N Engl J Med. 2018;378(9):829–839.
Dubin A, Otero J, Martín LC, et al. International Fluid Academy (IFA) recommendations. Ann Intensive Care. 2020;10(Suppl 1):79.
Wang Z, Zheng H, Deng J, et al. Hemorrhagic shock resuscitated with Ringer’s (bicarbonate vs lactate): randomized controlled trial. J Inflamm Res. 2022;15:6123–6133.
Xu J, Walline JH. Treatment of hyperkalemic emergencies. J Thorac Dis. 2022;14(5):1455–1462.
Farkas JD. Fluid selection & pH-guided fluid resuscitation. EMCrit Project. Updated Oct 2024. Accessed Dec 2025.
Jaber S, Paugam-Burtz C, Dupres G, et al. Sodium bicarbonate therapy in severe metabolic acidaemia in ICU: the BICAR-ICU randomized trial. Lancet. 2018;392:31–40.
Jung B, Jabaudon M, De Jong A, et al. Sodium bicarbonate for severe metabolic acidemia and acute kidney injury: the BICAR-ICU-2 randomized clinical trial. JAMA. 2025; e2520231.
Blank S, Blank R, Laupland K, et al. Sodium bicarbonate administration for metabolic acidosis in the ICU: target trial emulation. Intensive Care Med. 2025;51:1078–1086.
Sabatini S, Kurtzman N. Bicarbonate therapy in severe metabolic acidosis. J Am Soc Nephrol. 2009;20:692–695.
Fujii T, Udy AA, Licari E, et al. Sodium bicarbonate therapy in critically ill metabolic acidosis: review. J Crit Care. 2019;51:184–191.
Fujii T, Udy A, Nichol A, et al. International observational study of metabolic acidosis treatment with bicarbonate in ICU. Crit Care. 2021;25:108.
Arieff AI. Indications for bicarbonate use in metabolic acidosis. Br J Anaesth. 1991;67:165–177.
Yang T, Lin H, Wang H, et al. Sodium bicarbonate treatment and outcomes in CKD with metabolic acidosis. Clin J Am Soc Nephrol. 2024;19:959–969.
Tong L, Wu S, Li D, et al. Hyperchloremic acidosis benefiting from sodium bicarbonate therapy. Eur J Intern Med. 2024.
Navaneethan S, Shao J, Buysse J, Bushinsky DA. Treating metabolic acidosis in CKD: systematic review. Clin J Am Soc Nephrol. 2019;14:1011–1020.
Beautiful explanations and references!
Beautifully summarised and debunked the myths