Beyond Bundles: How the 2026 Sepsis Guidelines Redefine Acute Care?
Practical bedside wisdom distilled from the 2026 Surviving Sepsis Campaign guidelines

This isn’t just an update
At first glance, the 2026 Surviving Sepsis Campaign guidelines look familiar.
Same bundles. Same urgency. Same resuscitation priorities.
But look closer.
This is not a routine revision.
It’s a philosophical shift — from protocol-driven sepsis care to context-aware, system-level, precision acute care.
And if you work in the emergency department or ICU, this changes how you think — not just what you do.
Follow us on Instagram: @humans.of.em
What Changed (and Why It Matters)
1. Sepsis is now a system problem, not just a bedside problem
2026:
Performance improvement programs + quality improvement (QI)
→ Strong recommendation, moderate certainty of evidenceIntroduction of:
“Code sepsis” / sepsis huddle
→ Conditional recommendation, low certainty
2021:
Performance programs recommended
→ Strong, moderate-quality evidence (screening)
What changed?
QI is no longer administrative — it’s therapeutic.
Acute care takeaway:
You’re not just treating septic shock anymore.
You’re part of a hospital-wide intervention system.
2. Antibiotics: The death of the “1-hour rule for everyone”
2021:
Antibiotics within 1 hour for all sepsis
→ Strong recommendation (low/very low evidence)
2026:
Septic shock / high suspicion → immediate antibiotics
Possible sepsis (no shock) → investigate, give within 3 hours
Low likelihood → defer antibiotics
👉 Evidence:
Strong (shock)
Weak / very low (non-shock)
Why this matters:
A major pivot toward antimicrobial stewardship
Acute care reality:
You now need to balance:
Delay = harm
Overuse = harm
That’s a harder — and more honest — guideline.
👉 Dosing strategy finally gets attention
Prolonged infusion of beta-lactams over bolus dosing
→ Weak recommendation, moderate-quality evidence
Why this matters
Aligns with PK/PD principles
Improves time above MIC, especially in:
Septic shock
Altered pharmacokinetics
Practical takeaway
Start thinking beyond “which antibiotic”
Move toward:
👉 How you give it matters as much as what you give
Antibiotics don’t just start early — they must stop early
👉 Daily assessment for de-escalation based on culture and susceptibility
→ Weak recommendation, very low-quality evidence
👉 Avoid prolonged broad-spectrum therapy once pathogen is identified
Why this matters
This is a major philosophical shift:
Earlier guidelines focused on early administration
2026 emphasizes early de-escalation
Acute care takeaway
Antibiotics are not a one-time decision
They are a dynamic therapy
👉 Start broad (when needed)
👉 Narrow early (when possible)
3. Screening: Less faith in qSOFA, more in broader tools
2021:
Against using qSOFA alone
→ Strong recommendation, moderate-quality evidence
2026 reinforces and clarifies:
👉 Use NEWS, NEWS2, MEWS, or SIRS over qSOFA as a single screening tool
→ Strong recommendation, moderate certainty of evidence
Also adds:
Prehospital screening
→ Conditional, very low evidence
Why this matters
qSOFA was attractive because it was simple.
But simplicity came at the cost of sensitivity.
👉 The 2026 guideline firmly moves away from qSOFA as a standalone tool.
Acute care takeaway
Stop relying on qSOFA alone
Use early warning scores + clinical judgment
Screening is not a number — it’s a system + process
4. Fluids: The quiet downgrade
2021:
30 ml/kg fluids
→ Weak recommendation, low-quality evidence (downgraded)
2026 direction:
Reinforces individualized resuscitation
Moves away from rigid fluid mandates
Takeaway:
The guideline no longer believes in “one-size-fits-all fluids”
5. Lactate, CRT, and monitoring: still here, still weak
Lactate-guided resuscitation
→ Weak, low-quality evidenceCapillary refill time
→ Weak evidence
Translation:
We use them.
We trust them.
But the evidence is still not strong.
6. Adjuncts: Less enthusiasm, more skepticism
Strong:
No starch → Strong, high-quality evidence
Norepinephrine first-line → strong
Weak / against:
Vitamin C → Weak against
Hemoperfusion → Weak against
Pattern:
Most adjuncts either:
Don’t work
Or don’t have good evidence
7. Ventilation: One of the few stable areas
Low tidal volume → Strong, high-quality evidence
Proning → Strong, moderate-quality evidence
HFNC over NIV → Weak, low-quality evidence
Insight:
Respiratory care remains one of the most evidence-consistent domains
8. New emphasis: survivorship and transitions of care
2026 expands into:
Goals of care discussions
Post-sepsis syndrome
Transitions of care
Mostly:
👉 Best practice / weak evidence
Shift:
Sepsis is no longer an ICU event.
It is a longitudinal disease process
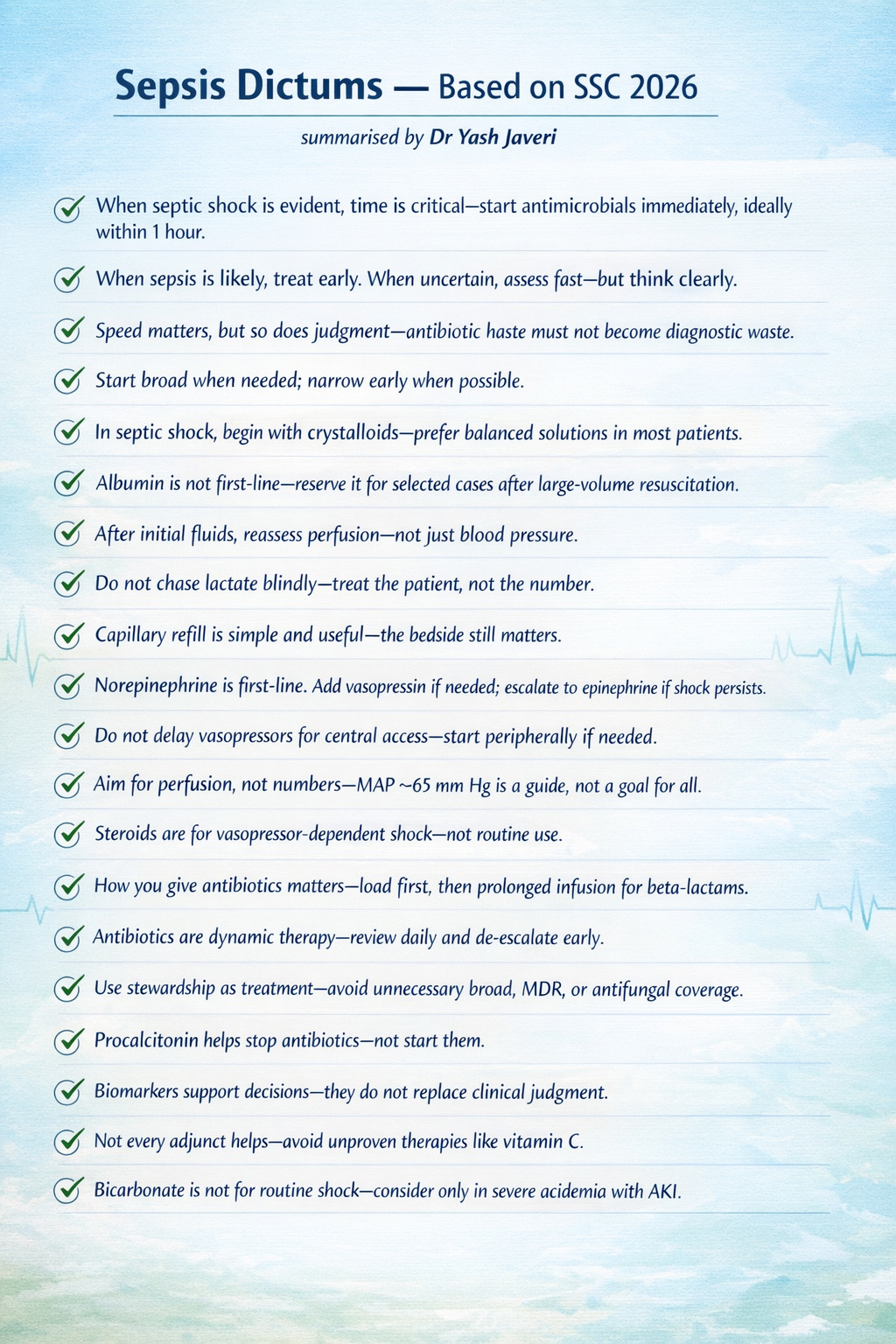
If you remember only few things from 2026:
Think before antibiotics (unless shock)
How you give antibiotics (infusion strategy) matters
De-escalate early — stewardship is core care
Fluids are individualized, and type matters
What This Means: A Critical Appraisal
a). The uncomfortable truth: Evidence is still weak
Across domains:
Antibiotics (non-shock) → very low certainty
Fluids → low certainty
CRT/lactate → low certainty
Code sepsis → low certainty
👉 Despite decades of research, high-certainty evidence is limited
b). The “GRADE paradox”
The guideline uses structured GRADE methodology:
“We recommend” → strong
“We suggest” → conditional
But:
👉 Strong recommendations sometimes sit on low-quality evidence (especially earlier guidelines)
👉 Many new recommendations remain conditional
💡 Implication:
This is transparent science — but still uncertain medicine
c). From protocols → clinical judgment
Old era:
Bundles
Timelines
Protocol compliance
2026:
Diagnostic probability
Stewardship
Context-aware decisions
This is the real shift:
The guideline now expects thinking, not just following
d). The antibiotic pivot is the most practice-changing update
Before:
Everyone gets antibiotics early
Now:
Timing depends on:
Severity
Probability of infection
Clinical reality:
You are now balancing:
Sepsis mortality vs antimicrobial harm
This is harder — but more accurate.
e). Real-world applicability (especially LMIC settings)
The guideline acknowledges:
Resource variability
Need for adaptable systems
💡 Interpretation:
“Code sepsis” may help more in chaotic, resource-limited systems
Protocols alone don’t fix outcomes without infrastructure
f). The deeper truth: Sepsis remains poorly understood
Even in 2026:
Few high-certainty interventions
Many weak recommendations
Heavy reliance on physiology and pragmatism
👉 Sepsis is still a syndrome, not a single disease
The 2026 Surviving Sepsis Guidelines don’t give you more answers.
They give you better questions.
And in the resuscitation bay at 3 AM —
that might be exactly what we needed.