
Asymptomatic Elevated Blood Pressure in the Emergency Department
What the Evidence Actually Says — and When (Rarely) to Treat

Every emergency physician encounters this scenario:
A patient presents for a minor complaint.
Vitals show BP 186/108 mmHg.
They look comfortable. No red flags.
The reflex question follows:
“Should we lower this before discharge?”
According to current evidence: usually no — and sometimes doing so causes harm.¹
Why Terminology Matters
The 2024 American Heart Association (AHA) Scientific Statement strongly discourages emotive terms like “hypertensive urgency” because they drive unnecessary treatment cascades.¹
Instead, use objective categories:
1. Asymptomatic Elevated BP
SBP ≥130 or DBP ≥80 mmHg
No symptoms
No evidence of acute target-organ damage
2. Asymptomatic Markedly Elevated BP
SBP >180 or DBP >110–120 mmHg
Patient feels well
No acute organ injury
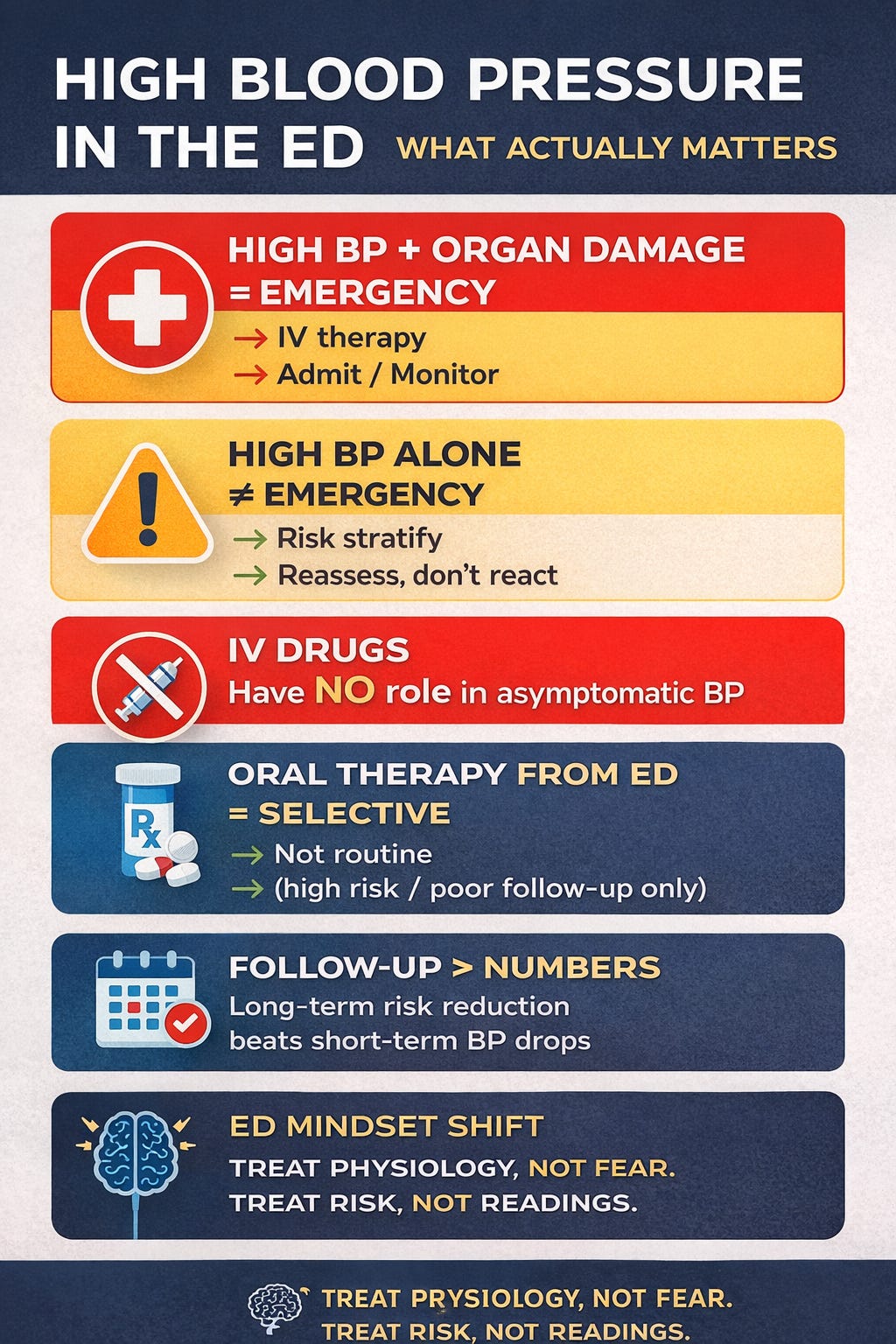
3. Hypertensive Emergency
Any BP
Plus acute target-organ damage
➡️ Only hypertensive emergency requires urgent BP reduction (usually IV).
Before Calling It “Asymptomatic”: What Must Be Ruled Out
A patient is not asymptomatic until acute end-organ injury is excluded.
Target-organ damage to actively assess (BARKH framework¹):
Brain
Stroke, TIA
Hypertensive encephalopathy
Intracranial hemorrhage
PRES
Heart
Acute coronary syndrome
Acute heart failure / pulmonary edema
Myocardial injury
Arteries
Aortic dissection
Kidneys
Acute kidney injury
Thrombotic microangiopathy
Retina
Acute visual changes and Grade III–IV hypertensive retinopathy
If any of the above are present → this is not asymptomatic BP and must be managed as a hypertensive emergency.¹,²
First-Time High BP vs Known Hypertension
This distinction matters.
First-Time Elevated BP
Common in ED due to pain, anxiety, illness, sleep deprivation
Single ED reading does not diagnose hypertension
Diagnosis requires out-of-office or repeated measurements¹,²
➡️ For first-time high BP without organ damage:
Do not label
Do not treat acutely
Do ensure follow-up
Known Hypertension
Check medication adherence
Restart home meds if omitted during illness or admission¹
Persistent, markedly elevated readings may justify selective treatment only in high-risk or poorly followed patients¹,³
Confirm the Number Before Reacting
ED BP readings are frequently inaccurate.¹
Before acting:
Repeat BP after 5–10 minutes of rest
Use correct cuff size and positioning
Address pain, anxiety, bladder distension
Review drugs that raise BP (NSAIDs, steroids, stimulants)
The AHA emphasizes that measurement error alone accounts for many “severe” readings.¹
What Not to Do (Strong Evidence of Harm)
For asymptomatic elevated or markedly elevated BP:
❌ IV antihypertensives
❌ Rapid BP lowering
❌ PRN parenteral agents
❌ Treating numbers without physiology
Observational studies consistently show higher rates of hypotension, AKI, myocardial injury, stroke, and mortality when asymptomatic BP is treated aggressively in acute care.¹,⁴–⁶
The Default ED Strategy
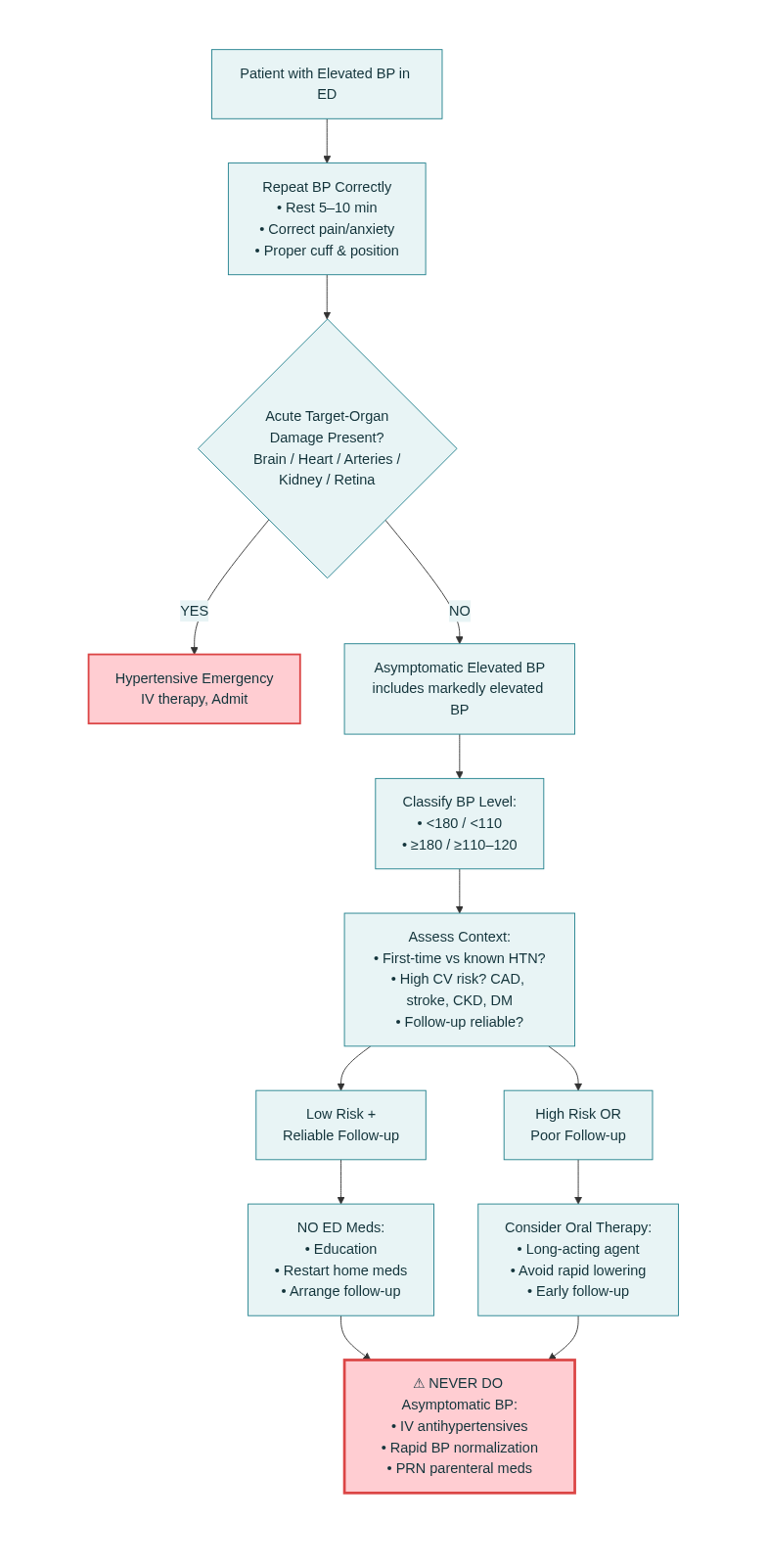
When Does Starting Oral Therapy From the ED Make Sense?
Treatment should be the exception, not the rule.¹
Consider oral antihypertensives ONLY if:
Persistent BP ≥180/110–120 mmHg, despite rest
ANDFollow-up is unreliable (no PCP, high risk of loss to care)
ORPatient is high cardiovascular risk:
CAD, prior stroke, HF
CKD or diabetes
Persistently uncontrolled outpatient BP
If initiated:
Use long-acting oral agents
Avoid short-acting or rapid-onset drugs
Aim for gradual control, not normalization¹,³
References :
Bress AP, Anderson TS, Flack JM, et al. The management of elevated blood pressure in the acute care setting: A scientific statement from the American Heart Association. Hypertension. 2024;81:e94-e106.
Wolf SJ, Lo B, Shih RD, Smith MD, Fesmire FM. Clinical policy: Critical issues in the evaluation and management of adult patients in the ED with asymptomatic elevated blood pressure. Ann Emerg Med. 2013;62(1):59-68.
Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults. Hypertension. 2018;71:e13-e115.
Anderson TS, Herzig SJ, Jing B, et al. Clinical outcomes of intensive inpatient blood pressure management in hospitalized older adults. JAMA Intern Med. 2023;183(8):715-723.
Rastogi R, Sheehan MM, Hu B, et al. Treatment and outcomes of inpatient hypertension among adults with noncardiac admissions. JAMA Intern Med. 2021;181(3):345-352.
Ghazi L, Li F, Chen X, et al. Severe inpatient hypertension and blood pressure response to antihypertensive treatment. J Clin Hypertens. 2022;24:339-349.