
Aspiration ≠ Pneumonia: Why Antibiotics Are Often Unnecessary
A Regular Diagnosis We Keep Getting Wrong—and Why It Fuels Antibiotic Overuse

Aspiration-related lung injury is something we manage almost every day in emergency and acute care—after seizures, intoxication, stroke, vomiting, peri-intubation events, or in frail elderly patients with dysphagia.
Yet despite how common it is, aspiration pneumonitis and aspiration pneumonia are routinely conflated, leading to systematic overdiagnosis of infection, unnecessary antibiotics, broader spectra than required, and erosion of antimicrobial stewardship.¹–³
This is not a semantic distinction. These are two biologically distinct entities with different pathophysiology, natural history, and treatment implications.
Two Distinct Entities, One Common Mistake
Aspiration Pneumonitis (Chemical Injury)
Aspiration pneumonitis is a non-infectious inflammatory lung injury caused by inhalation of sterile gastric contents.
Typical features:
Often witnessed aspiration
Acute onset (within hours)
Hypoxemia, tachypnea, fever, leukocytosis
New infiltrates on imaging
Clinical improvement within 24–48 hours with supportive care alone⁴–⁷
Multiple studies demonstrate that empiric or prophylactic antibiotics do not improve outcomes and may increase adverse effects and resistance.⁴,⁷
Key point: Fever, leukocytosis, and infiltrates early after aspiration do not equal infection.
Aspiration Pneumonia (Infectious Disease)
Aspiration pneumonia is a true infectious process, caused by inhalation of oropharyngeal secretions colonized with pathogenic bacteria.
Typical features:
Often unwitnessed or silent aspiration
Delayed onset (>48 hours)
Persistent or worsening fever
Purulent sputum
Progressive radiographic infiltrates
Common in elderly, frail patients, stroke, neurologic disease, poor oral hygiene⁸–¹⁰
Only aspiration pneumonia requires antibiotics.
Why We Overdiagnose Aspiration Pneumonia ?
The problem is not under-recognition—it is overdiagnosis.
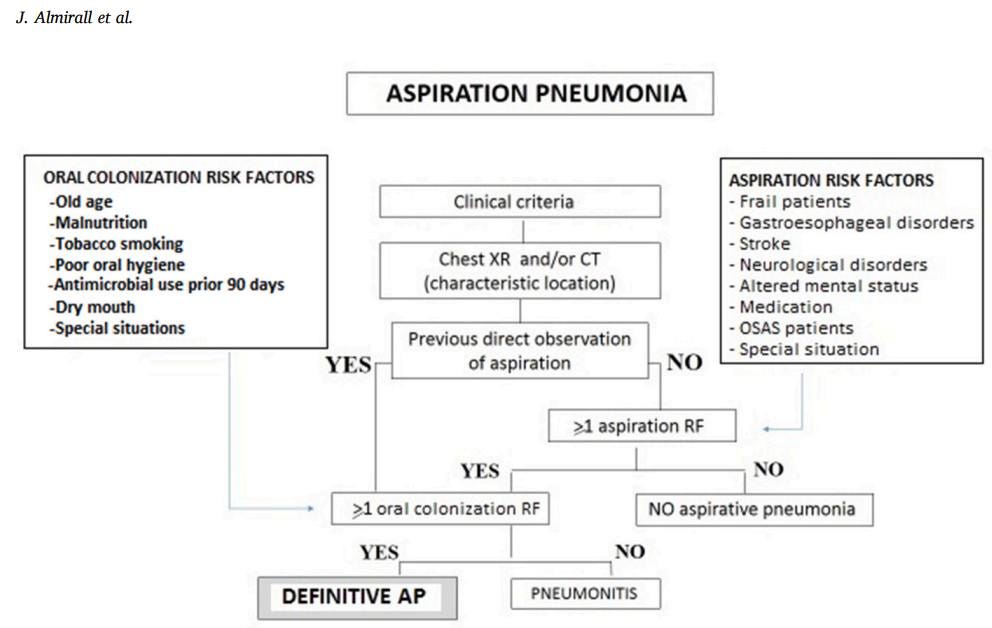
The 2021 Respiratory Medicine review by Almirall et al. clearly states that aspiration pneumonitis is frequently misdiagnosed and treated as infection, largely because clinicians “tend to consider all pulmonary complications of aspiration to be infectious”
Contributing factors include:
Early imaging misinterpretation – infiltrates occur in both entities.
Reflex antibiotic prescribing – aspiration + fever = antibiotics.
Fear of deterioration in elderly or critically ill patients.
Lack of a unified diagnostic framework, especially when aspiration is silent.
This diagnostic shortcut is one of the most common drivers of inappropriate antibiotic use in aspiration syndromes.
Imaging: Useful for Detection, Not Etiology
Chest X-ray and CT
Chest X-ray: gravity-dependent infiltrates
CT: bronchopneumonia pattern, centrilobular nodules, tree-in-bud
Neither modality can distinguish infection from chemical injury¹¹,¹⁴
Lung Ultrasound: A Powerful Tool with Important Limits
Lung ultrasound (LUS) has excellent diagnostic accuracy for pneumonia:
Sensitivity: ~86–99%
Specificity: ~81–98%
across multiple meta-analyses.¹⁵–²⁰
Typical findings:
Subpleural consolidations
Dynamic air bronchograms
B-lines
Pleural abnormalities¹⁵,¹⁶,²¹
Where LUS Fails Us
Aspiration pneumonitis produces identical ultrasound patterns—B-lines and subpleural consolidations—because LUS detects lung injury, not infection.²²–²⁵
LUS answers “Is there lung involvement?”—not “Is this infection?”
Using ultrasound findings alone to trigger antibiotics is a common stewardship error.
What Guidelines Actually Say About Antibiotics (And What We Ignore)
Both IDSA-aligned guidance and BMJ Best Practice state:
Empiric treatment of aspiration pneumonia should follow standard CAP/HAP/VAP regimens
Routine anaerobic coverage is NOT required
Anaerobic therapy is reserved only for:
Lung abscess
Empyema
Necrotizing pneumonia
Severe periodontal disease
Dysphagia or stroke alone does not justify anaerobic coverage
This directly contradicts the widespread ED practice of reflexively adding clindamycin or metronidazole after any aspiration event.
Almirall et al. further emphasise that initial antibiotic therapy is not indicated in chemical pneumonitis, and that failure to differentiate these entities leads to antibiotic overuse
References:
IDSA/ATS CAP Guidelines; BMJ Best Practice (Aspiration pneumonia, updated 2023);
Almirall J et al. Respiratory Medicine 2021
Antibiotics: When to Start—and When to Stop
Do NOT start antibiotics if:
Isolated aspiration event
Symptoms <48 hours
Improving oxygenation and clinical trajectory⁴,⁷,²⁶
Start empiric antibiotics if:
Symptoms persist or worsen beyond 48 hours
Progressive infiltrates
Purulent sputum, rising inflammatory markers
High-risk or critically ill patients (with mandatory reassessment)²⁶,
Early de-escalation is as important as initiation.
Why This Matters: The Stewardship Cost
Overuse of antibiotics in aspiration syndromes is associated with:
Increased multidrug-resistant organisms
Longer hospital stay
Higher complication rates
No mortality benefit¹–³,³¹
Aspiration syndromes represent a major, preventable source of inappropriate antibiotic exposure in emergency medicine.
REFERENCES
Friedman ND, Temkin E, Carmeli Y. The negative impact of antibiotic resistance. Clin Microbiol Infect. 2016;22:416-422.
Papadopoulos D, et al. Microbiology and prognosis of aspiration pneumonia. Le Infezioni in Medicina. 2018;26:103-114.
Saravolatz LD, et al. Empiric antibiotics and outcomes in pneumonia. Clin Infect Dis. 2025.
Dragan V, et al. Prophylactic antimicrobial therapy for acute aspiration pneumonitis. Clin Infect Dis. 2018;67:513-518.
Raghavendran K, et al. Aspiration-induced lung injury. Crit Care Med. 2011;39:818-826.
Goto A, et al. Aspiration pneumonitis not requiring antibiotics. Geriatr Gerontol Int. 2023;23:760-761.
Aga M, et al. Early antibiotics in aspiration pneumonitis. Intern Emerg Med. 2021;16:1841-1848.
Mandell LA, Niederman MS. Aspiration pneumonia. N Engl J Med. 2019;380:651-663.
Yoshimatsu Y, et al. Diagnosis of aspiration pneumonia in older persons. Eur Geriatr Med. 2022;13:1071-1080.
Almirall J, et al. Aspiration pneumonia: a renewed perspective and practical approach. Respir Med. 2021;185:106485.
Aspiration_pneumonia_A_renewed_…
Komiya K, Kadota J. CT features of aspiration pneumonia. Respir Investig. 2020.
Lascarrou JB, et al. Antibiotics after aspiration in ventilated patients. Crit Care Med. 2017;45:1268-1275.
Trujillo N, et al. Stewardship in critically ill CAP. Antimicrob Steward Healthc Epidemiol. 2025.
Ueda A, et al. CT findings in aspiration pneumonia. J Gen Fam Med. 2024;25:384-387.
Chavez MA, et al. Lung ultrasound for pneumonia diagnosis. Respir Res. 2014;15:50.
Reissig A, et al. Lung ultrasound in CAP. Chest. 2012;142:965-972.
Boccatonda A, et al. Infectious pneumonia and lung ultrasound. J Clin Med. 2023;12.
Metlay JP, et al. ATS/IDSA CAP guidelines. Am J Respir Crit Care Med. 2019;200:e45-e67.
Desai D, et al. Accuracy of lung ultrasound for pneumonia. Adv Respir Med. 2024;92:241-253.
Nufaiei Z, Alshamrani K. Ultrasound vs CXR vs CT. Med Devices. 2025;18:149-159.
Vaitheeswaran G, et al. POCUS lung ultrasound. Lung India. 2024;41:411-415.
Buonsenso D, et al. Aspiration pneumonia and lung ultrasound. J Ultrasound. 2020;25:325-331.
Yan Y, et al. Early diagnosis of aspiration pneumonia using LUS. Med Ultrason. 2024;26:104-105.
Soldati G, et al. Lung ultrasound artifacts. Expert Rev Respir Med. 2019;13:163-172.
DeSanti RL, et al. Lung ultrasound in respiratory failure. Pediatr Crit Care Med. 2021;22:722-732.
Moore FA. Treatment of aspiration in ICU patients. JPEN. 2002;26:S69-S74.
Lascarrou JB, et al. Differentiating pneumonitis from pneumonia. Crit Care Med. 2017;45:1268-1275.
Marín-Corral J, et al. Aspiration risk factors and empiric antibiotics. Chest. 2020.
Yoshimatsu Y, et al. Anaerobic coverage in aspiration pneumonia. J Clin Med. 2023;12.
Bai AD, et al. Anaerobic coverage: benefits and harms. Chest. 2024;166:39-48.
Pan D, Niederman MS. Therapy of aspiration. Semin Respir Crit Care Med. 2024.
IDSA/ATS CAP Guidelines; BMJ Best Practice (Aspiration pneumonia, updated 2023);
Almirall J, Boixeda R, de la Torre MC, Torres A.
Aspiration pneumonia: A renewed perspective and practical approach.
Respir Med. 2021;185:106485. doi:10.1016/j.rmed.2021.106485
When the standard of care is to treat every “positive” UA and lung infiltrate with 7d of IV antibiotics (starting minutes after the gastric acid hits the lungs), you become a major outlier trying to practice good medicine. It feels futile when someone will find the test a week later and still feel obliged to treat it. Not sure how we get to a new standard until AI baked into the EMR just does it for us.