
Albumin in the ED: When It Helps — and When It Doesn’t
A high-cost therapy with a narrow window of benefit

Albumin is far from a benign “better fluid” — it’s a high-cost therapy with very specific, evidence-based indications. In Emergency Medicine and critical care, albumin is not for simple “low albumin levels” or routine volume expansion.¹-³
Where Albumin Actually Works in Acute Care?
Strongest indications — supported by clinical trials + guidelines:
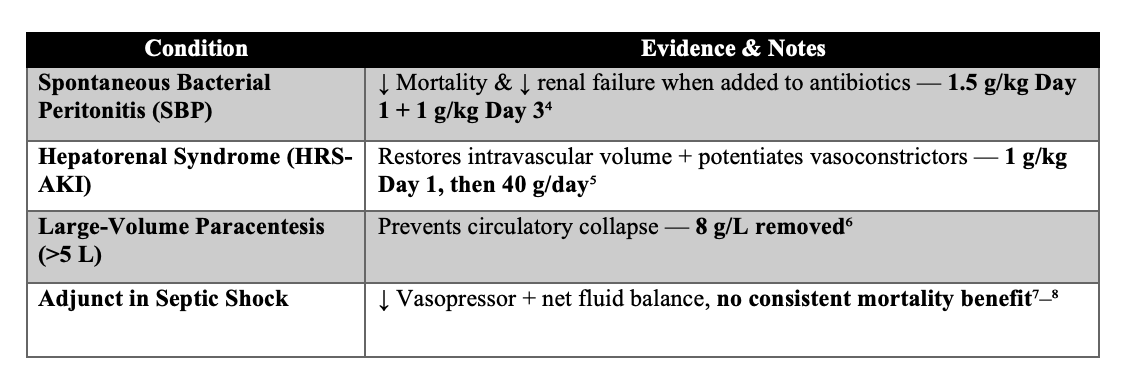
Overall benefits: Better hemodynamics.
Not proven to save lives in general sepsis population.
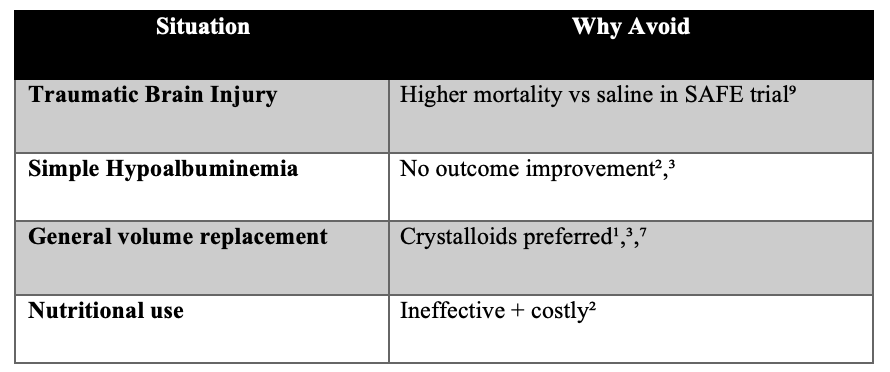
Where Albumin Should NOT Be Used ?
⚠️ Safety & Contraindications
Volume overload with 5% albumin (caution in HF/renal failure)
Worse outcomes in TBI (avoid completely)⁹
Monitor for: pulmonary edema, AKI, allergic reactions
Very cost-intensive misuse in EDs³
Pearl: If a patient is not intravascularly depleted, albumin won’t help.
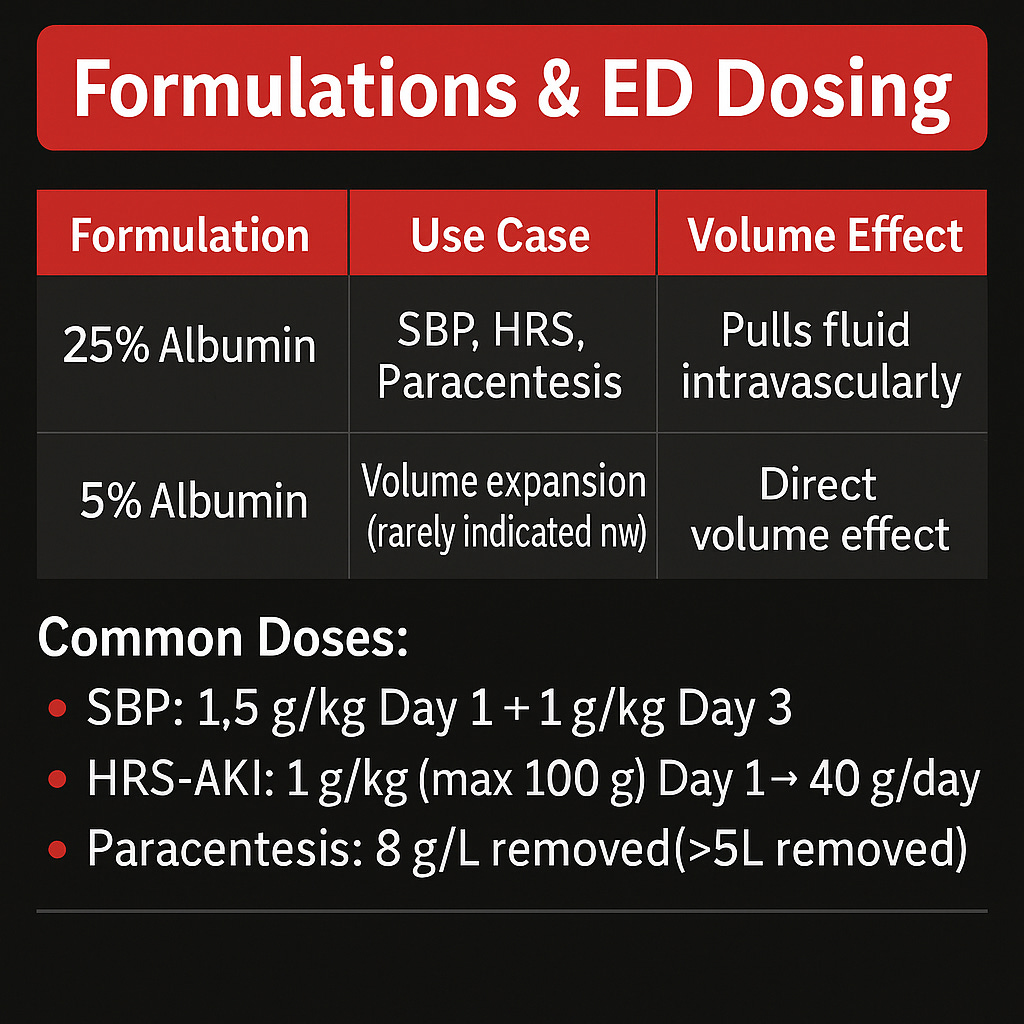
Formulations
25% Albumin ==> SBP, HRS, Paracentesis ===> Pulls fluid intravascularly
5% Albumin ==> Volume expansion (rarely indicated now) ===>Direct volume effect
Common Doses:
SBP: 1.5 g/kg Day 1 + 1 g/kg Day 3⁴
HRS-AKI: 1 g/kg (max 100 g) Day 1 → ~40 g/day⁵
Paracentesis: ≥8 g/L removed⁶
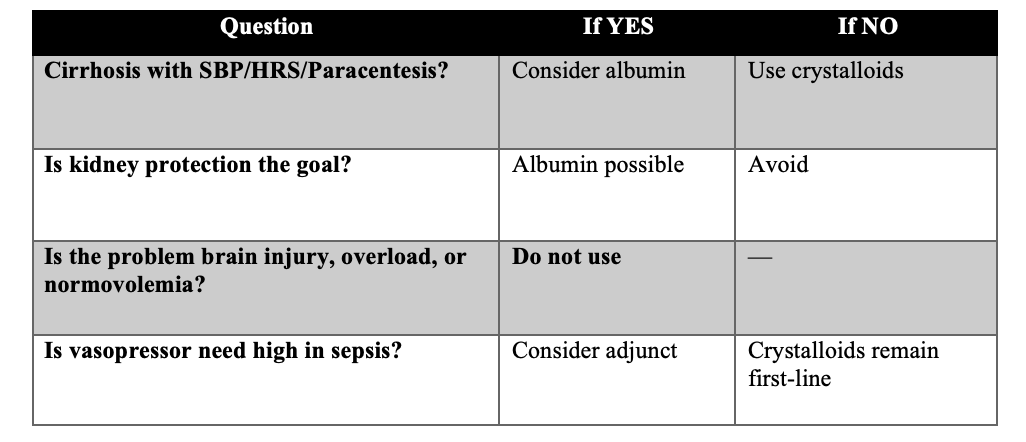
ASK THESE QUESTIONS BEFORE ORDERING:
Evidence Recap — Key Trials & Guidelines
SAFE Trial (2004): No mortality benefit to albumin; harm in TBI
Sort et al. (1999): Survival benefit in SBP with albumin + antibiotics
ICM Guideline 2024: Do NOT use albumin for routine resuscitation or hypoalbuminemia
ICARUS-ED 2025: Ongoing interest as adjunct in severe sepsis — signals but not definitive

References :
Abedi F, Zarei B, Elyasi S. Albumin: a comprehensive review and practical guideline for clinical use. Eur J Clin Pharmacol. 2024. doi:10.1007/s00228-024-03664-y
Wiedermann CJ. Human Albumin Infusion in Critically Ill and Perioperative Patients: Rapid Review. J Clin Med. 2023;12. doi:10.3390/jcm12185919
Moomey K, Gurnani P. ALBUMIN-IMIZE: Characterizing Intravenous Albumin Use. Crit Care Med. 2018;46:573. doi:10.1097/01.ccm.0000529183.05206.6d
Sort P, Navasa M, Arroyo V, et al. Effect of IV albumin on SBP–associated renal impairment. N Engl J Med. 1999;341(6):403-409. doi:10.1056/NEJM199908053410603
Guevara M, Fernandez-Seara J, et al. Albumin for hepatorenal syndrome. Hepatology. 2012;56:1362-1372. PMID: 31723234
Runyon BA. Management of Adult Patients With Ascites Due to Cirrhosis. Hepatology. 2009;49:2087-2107. (Paracentesis guideline)
Williams J, Greenslade J, Hills A, Ray M. ICARUS-ED trial. Ann Emerg Med. 2025. doi:10.1016/j.annemergmed.2024.12.016
International Collaboration for Transfusion Medicine. Albumin guideline. 2024; PMID: 38447639
SAFE Study Investigators. Saline vs Albumin Fluid Evaluation Trial. N Engl J Med. 2004;351:129-142. PMID: 15163774
Farkas JD. Albumin & fluid strategy. EMCrit Project – IBCC. 2024. https://emcrit.org/ibcc/fluid/#albumin
So in patients with CLD with hypoalbuminemia but without SBP or HRS or paracentesis is Albumin not indicated?