
Acute Pulmonary Embolism, Part 2: Treatment, Disposition, and Preventing Collapse
Applying the A–E classification to anticoagulation, reperfusion, monitoring, and follow-up in the emergency department

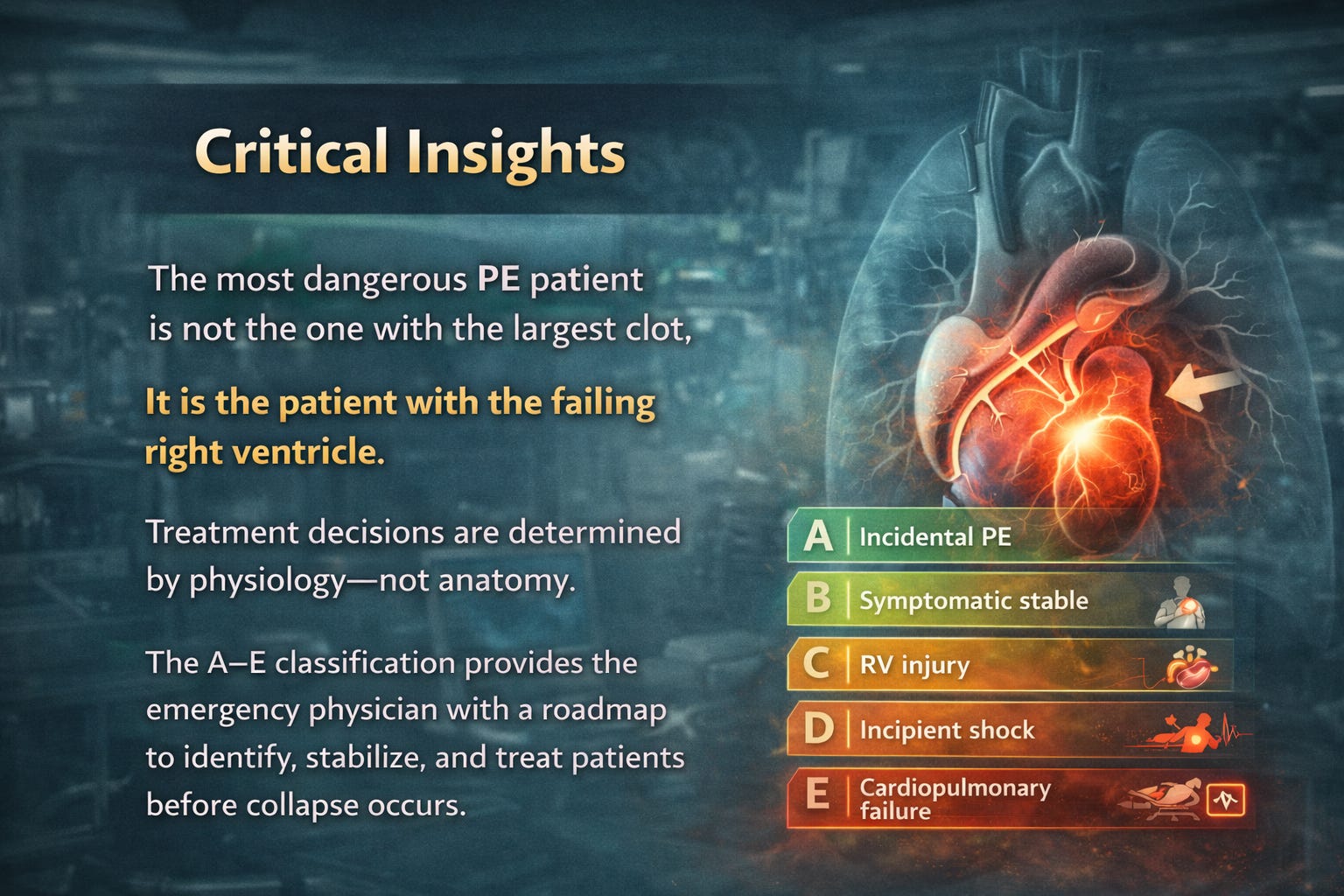
Pulmonary embolism does not kill by clot burden.
It kills by right ventricular failure.
The role of the emergency physician is not simply to diagnose PE—but to identify which patient will deteriorate, which patient needs reperfusion, and which patient can safely go home.
The 2026 AHA/ACC/ACEP classification (A–E) provides a physiology-based roadmap for treatment escalation, monitoring, and disposition.
This is where classification becomes action.
Step 1: Immediate ED Stabilization
COR 1, LOE B-NR
Initial management priorities in suspected or confirmed PE:
• Oxygenation
• Circulatory support
• RV perfusion preservation
• Prevention of hemodynamic collapse
Key immediate assessments:
• Blood pressure
• Oxygen requirement
• Lactate
• Mental status
• RV function
Patients in Category D or E require immediate resuscitation.
Oxygen and Respiratory Support
COR 1, LOE C-LD
Indicated in hypoxemic patients.
Target:
SpO₂ ≥ 90%-94%
Preferred escalation:
Nasal cannula
High-flow nasal oxygen
Non-invasive ventilation
Avoid unnecessary intubation.
Positive pressure ventilation reduces venous return and worsens RV failure.¹
If intubation unavoidable:
• Use hemodynamically stable induction agents
• Initiate vasopressors first
—> Physiologically difficult airway modification, give RV supporting ionotropes.
Circulatory Support
COR 1, LOE B-NR
Hypotension reflects RV failure and impaired cardiac output.
First-line vasopressor:
Norepinephrine
Benefits:
• Improves coronary perfusion
• Improves RV contractility
• Improves systemic vascular resistance¹
Avoid aggressive fluid boluses.
Excess fluid worsens RV dilation and reduces LV filling.
Step 2: Anticoagulation — The Foundation of Treatment
Anticoagulation prevents clot propagation and allows endogenous fibrinolysis.
COR 1, LOE A
Anticoagulation is recommended in all patients with confirmed PE unless contraindicated.¹
Choice of Anticoagulant
DOACs preferred in stable patients
COR 1, LOE A
Preferred agents:
• Apixaban
• Rivaroxaban
Advantages:
• Lower bleeding risk
• Rapid onset
• No monitoring required
• Suitable for outpatient treatment¹
LMWH preferred when inpatient management required
COR 1, LOE B-R
Preferred in:
• Hospitalized patients
• Cancer-associated thrombosis
• Moderate-risk PE¹
Advantages:
• Predictable anticoagulation
• Lower HIT risk
UFH preferred in unstable patients
COR 1, LOE B-NR
Indications:
• Category C3
• Category D
• Category E
• Planned thrombolysis or thrombectomy¹
Reason:
Rapid reversibility.
Step 3: Reperfusion Therapy
Indicated in RV failure and shock
Reperfusion reduces RV afterload and restores circulation.
Systemic Thrombolysis
COR 1, LOE B-R
Indicated in:
Category E1 — cardiogenic shock
Category E2 — cardiac arrest¹
Reduces mortality and improves hemodynamics.
Consider thrombolysis in Category D
COR 2a, LOE B-NR
Indicated if evidence of:
• Normotensive shock
• Elevated lactate
• Progressive hypoxia
• RV dysfunction¹
These patients are at high risk of deterioration.
Not recommended routinely in Category C
COR 3, LOE B-R
Routine thrombolysis in stable patients increases bleeding risk without mortality benefit.
Alteplase (tPA) Dose for Acute Pulmonary Embolism
Standard dose for high-risk PE (massive PE with shock)
Dose: 100 mg IV over 2 hours
Regimen:
100 mg alteplase IV infusion over 120 minutes
No bolus required (standard regimen)
This is the FDA-approved and guideline-recommended dose.
Alternative accelerated regimen (commonly used in ED / ICU)
Dose: 0.6 mg/kg IV over 15 minutes (max 50 mg)
Used when:
Rapid hemodynamic collapse
Need for faster reperfusion
Peri-arrest or severe shock
Evidence shows similar efficacy with potentially lower bleeding risk.
Alteplase Dose During Cardiac Arrest due to PE
When PE is suspected or confirmed cause of arrest:
Recommended regimen (AHA cardiac arrest guidance)
50 mg IV bolus over 2–5 minutes
Then:
Continue CPR for at least 15–30 minutes
If no ROSC, may repeat another 50 mg bolus after 15–30 minutes
Maximum total dose: 100 mg
Most commonly used cardiac arrest protocol in emergency medicine
Option 1 (most widely used):
Alteplase 50 mg IV push
Continue CPR 15–30 min
Repeat 50 mg if needed
Option 2 (alternative):
Alteplase 100 mg IV bolus over 10 minutes
Used less commonly due to bleeding risk.
Catheter-Directed Therapy
COR 2a, LOE B-NR
Indicated when:
• Thrombolysis contraindicated
• Failed thrombolysis
• Progressive deterioration¹
Advantages:
• Lower bleeding risk
• Targeted therapy
Mechanical Thrombectomy
COR 2a, LOE B-NR
Indications:
• Category D or E
• Contraindication to thrombolysis
• Failed thrombolysis¹
Improves hemodynamics rapidly.
Increasingly used in modern PE management.
ECMO
COR 2a, LOE C-LD
Indicated in refractory shock or cardiac arrest.
Provides circulatory support until reperfusion effective.
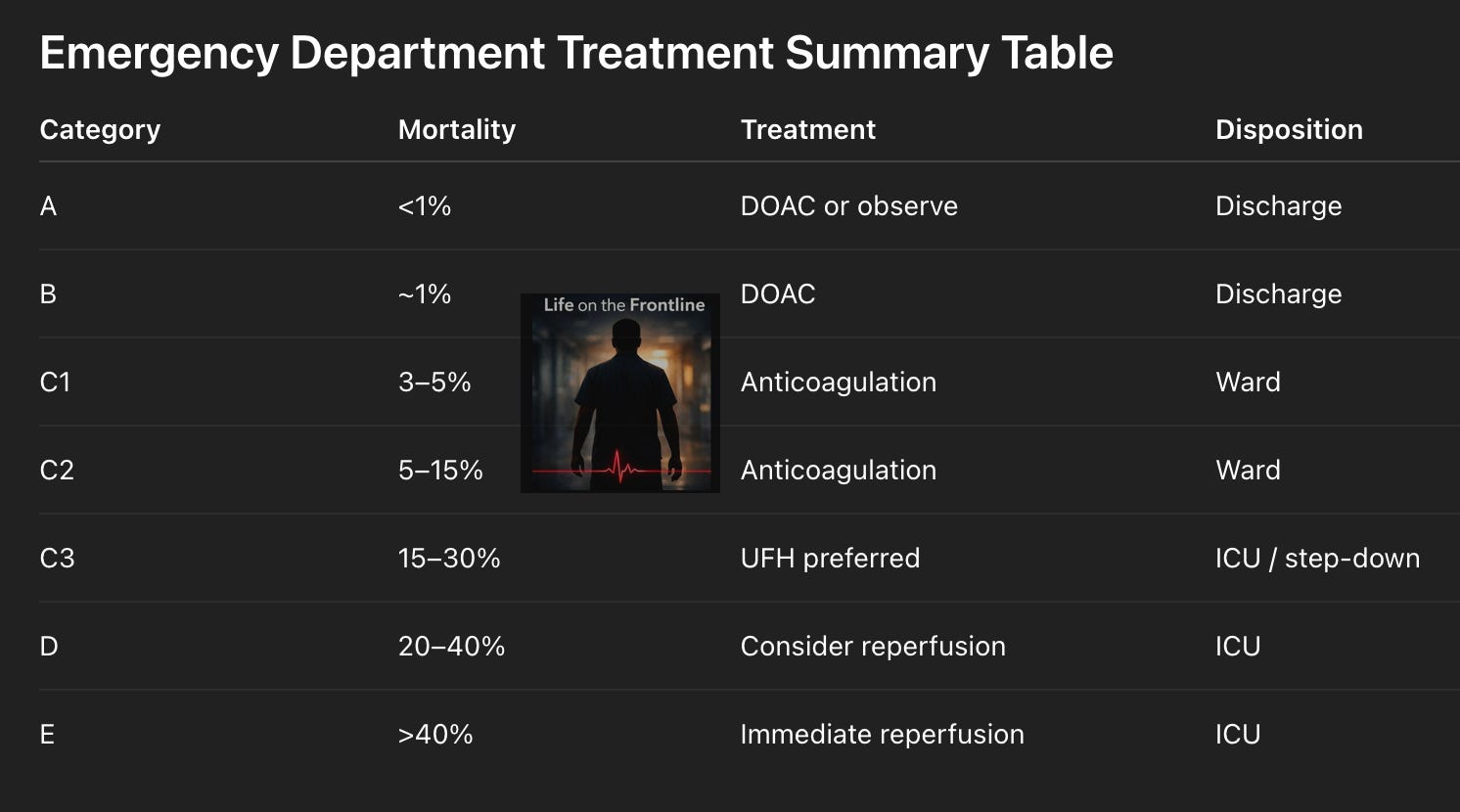
Step 4: Treatment and Disposition by A–E Group
This is the most important ED decision.
Category A — Incidental PE
Mortality risk: <1%
Treatment:
Anticoagulation or observation depending on risk factors¹
Disposition:
Discharge with outpatient follow-up
Category B — Symptomatic, Low Risk
Mortality risk: ~1%
Treatment:
DOAC preferred¹
Disposition:
Outpatient management recommended
Criteria:
• Stable vitals
• No hypoxia
• Reliable follow-up¹
Category C1 — Intermediate Risk, No RV Injury
Mortality risk: 3–5%
Treatment:
Anticoagulation¹
Disposition:
Hospital admission, telemetry
Category C2 — RV Injury or Biomarker Elevation
Mortality risk: 5–15%
Treatment:
Anticoagulation
Disposition:
Hospital admission with monitoring¹
Category C3 — RV Injury + Biomarker Elevation
Mortality risk: 15–30%
Treatment:
UFH preferred
Consider reperfusion if deterioration¹
Disposition:
Step-down or ICU
PERT consultation recommended.
Category D — Normotensive Shock
Mortality risk: 20–40%
Treatment:
UFH
Consider thrombolysis or thrombectomy¹
Disposition:
ICU
Immediate specialist consultation required.
Category E — Cardiogenic Shock or Arrest
Mortality risk: >40%
Treatment:
Immediate reperfusion therapy¹
Options:
• Thrombolysis
• Thrombectomy
• ECMO
Disposition:
ICU
Medical emergency.
Step 5: Monitoring
COR 1, LOE B-NR
Monitor for deterioration:
• Blood pressure
• Oxygen requirement
• Heart rate
• Lactate
• Mental status¹
Serial reassessment essential.
Patients may deteriorate rapidly.
Step 6: Complications and Sequelae
Acute complications
Right ventricular failure
Cardiogenic shock
Cardiac arrest
Primary causes of death.
Chronic thromboembolic pulmonary hypertension (CTEPH)
Occurs in 2–4% of patients.¹
Caused by persistent pulmonary vascular obstruction.
Symptoms:
• Progressive dyspnea
• Exercise intolerance
Post-PE syndrome
Occurs in up to 50% of patients.¹
Symptoms:
• Dyspnea
• Reduced exercise tolerance
• Functional impairment
Step 7: Duration of Anticoagulation
COR 1, LOE A
Minimum duration:
3 months¹
Extended anticoagulation recommended if:
• Unprovoked PE
• Persistent risk factors¹
I break down emergency medicine physiology visually and practically.
If you’re an emergency physician, resident, or acute care clinician, you’ll find additional diagrams, algorithms, and case-based insights here:
→ Follow on Instagram: @humans.of.em
This is where most of my visual teaching lives.
Reference
American College of Cardiology/American Heart Association Joint Committee. 2026 AHA/ACC guideline for the diagnosis and management of acute pulmonary embolism. J Am Coll Cardiol. 2026.
"UFH preferred in unstable patients": where did you read this statement in AHA guidelines? I missed
insightful
What about use of tenecteplase and streptokinase in thrombolysis?