
Acute Hyperkalemia: What Actually Works (With and Without ECG Changes)
A practical, evidence-based guide for frontline clinicians

Acute hyperkalemia is one of the few emergencies where treatment decisions must be made within minutes, often with incomplete information and subtle ECG findings. Yet management remains inconsistent — especially regarding the use of calcium, bicarbonate, and diuretics, with or without ECG changes.
This post breaks down what the evidence actually supports — without myths, without outdated dogma, and without unnecessary steps.
1. ECG Changes Drive the First Decision
When adequate ECG Changes Are Present
Immediate IV calcium (gluconate or chloride) is indicated.
Why?
It stabilizes cardiac myocytes and prevents malignant arrhythmias.
Calcium’s mechanism being reconsidered (Piktel 2024) - not membrane stabilisation
Time to effect: 1–3 minutes
Effect on potassium: None
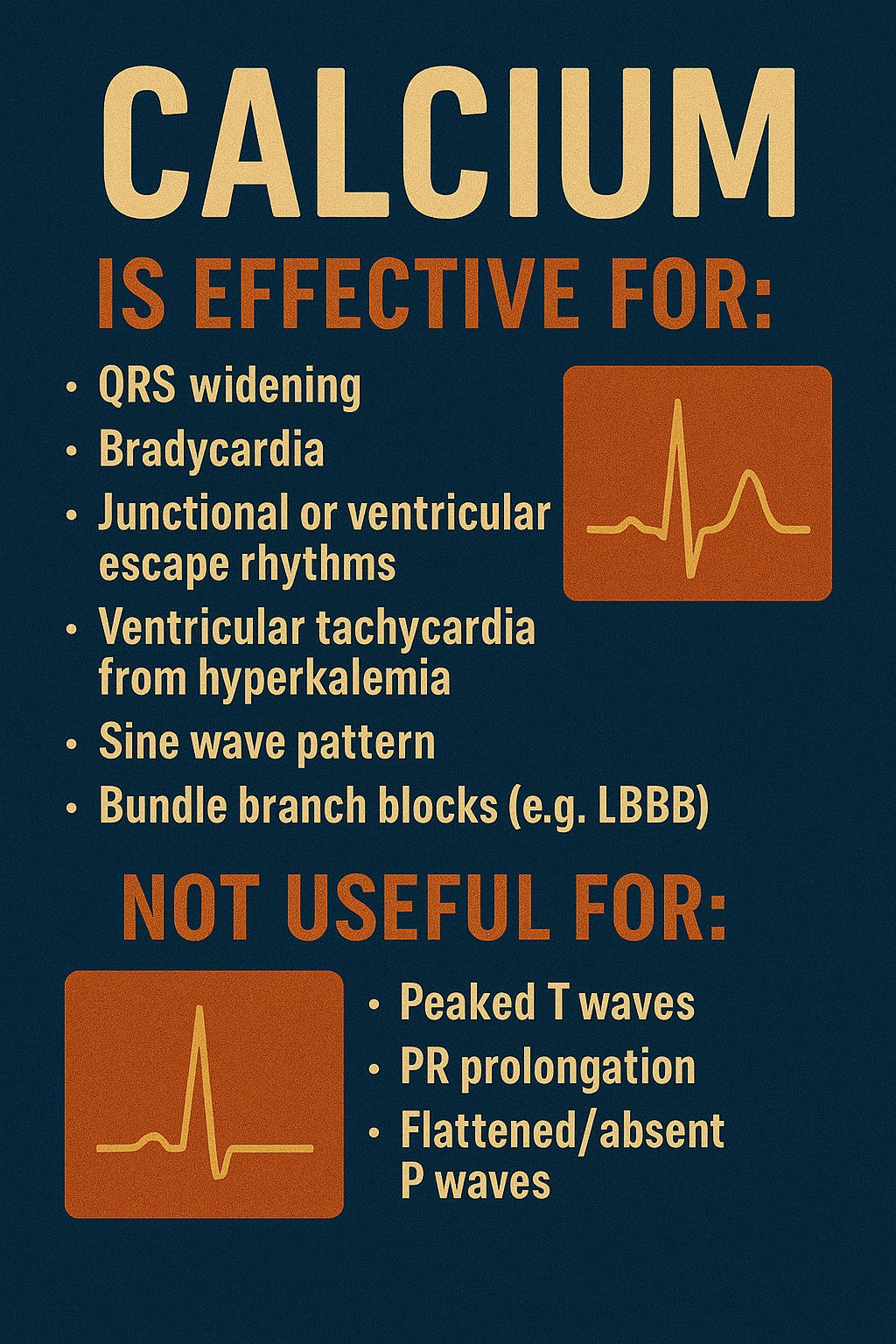
Calcium is effective for:
QRS widening
Bradycardia
Junctional or ventricular escape rhythms
Ventricular tachycardia from hyperkalemia
Sine wave pattern
Bundle branch blocks (e.g., LBBB)
Not useful for:
Peaked T waves
PR prolongation
Flattened/absent P waves
(Yamanoglu 2022; Durfey 2017; Bonar 2022; Lindner 2020)
This distinction is critical — calcium treats conduction and rhythm instability, not early repolarization changes.
When There Are No ECG Changes
Calcium is generally not indicated, and management focuses on:
✔ shifting potassium intracellularly
✔ removing potassium from the body
✔ treating the underlying cause
(Gupta 2021; Lindner 2020)
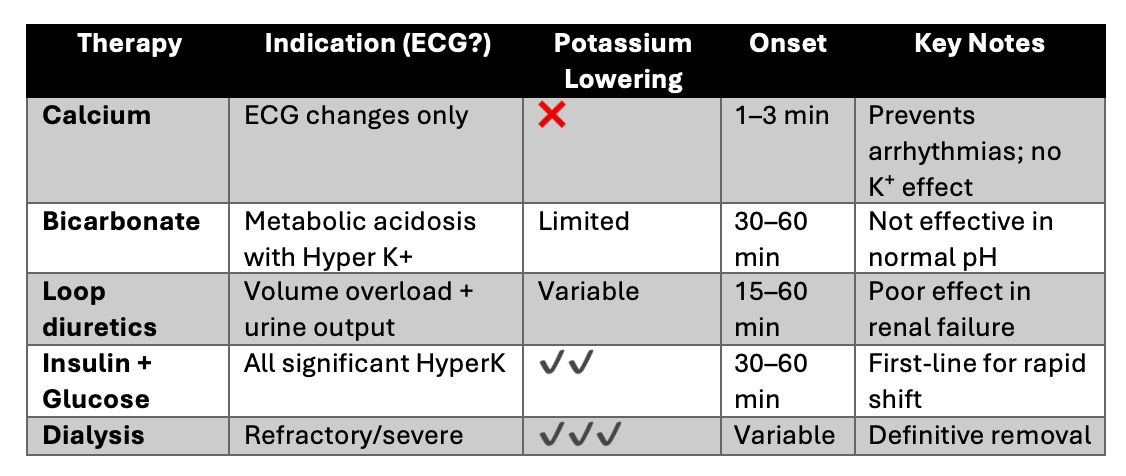
2. Comparing Key Therapies: What Each Actually Does
A) Calcium Salts
Role: Cardiac membrane stabilization
Indication: Only hyperkalemia with ECG abnormalities
Effect on K⁺: None
Risks: Hypercalcemia; caution in digitalis toxicity
The main point: calcium buys time, but it doesn’t fix the potassium.
B) Sodium Bicarbonate
Evidence shows bicarbonate has little to no potassium-lowering effect unless significant metabolic acidosis is present.
Indication: Severe metabolic acidosis
Usefulness: Limited in normal pH
Risks: Hypernatremia, fluid overload, venous irritation
(Jessen 2025; Geng 2021; Abuelo 2017; Dépret 2019)
C) Loop Diuretics
Loop diuretics (e.g., furosemide) promote renal potassium excretion, but only in patients who:
✔ have urine output
✔ have adequate renal function
✔ can tolerate fluid shifts
Effectiveness: Variable and unpredictable
Not useful: Severe renal dysfunction or anuric patients
(Dépret 2019; Lindner 2020; Wu 2023)
3. The Therapies That Actually Lower Potassium Fast
These remain the core of hyperkalemia management:
Insulin + Glucose
Most consistent and rapid intracellular shift
Drop: ~0.7–1.2 mmol/L in 1 hour
Risk: Hypoglycemia (monitor closely)
Beta-2 Agonists (e.g., nebulized salbutamol)
Additive effect when combined with insulin
Less effective as monotherapy
Dialysis
Definitive treatment, especially in:
severe renal dysfunction
refractory hyperkalemia
life-threatening situations
(Jessen 2025; Rafique 2021; Sun 2024)
5. What the Evidence Still Lacks
No standardized definition of “ECG changes”
Wide practice variation
Bicarbonate still used reflexively despite limited evidence
Loop diuretics often overestimated in renal dysfunction
Calcium’s mechanism being reconsidered (Piktel 2024)
The management framework remains solid, but practice inconsistencies persist.
Summary
The approach to acute hyperkalemia in the acute settings must be fast, structured, and ECG-informed.
✔ Give calcium ONLY if there are ECG conduction or rhythm abnormalities
✔ Do NOT rely on bicarbonate unless the patient is acidotic
✔ Diuretics work only if kidneys work
✔ Insulin + glucose remains the fastest and most reliable potassium-lowering therapy
✔ Dialysis is the definitive option for refractory or severe cases
Hyperkalemia is common — but mismanagement is too.
A clear, evidence-guided approach prevents dangerous delays and unnecessary interventions.
References
Abuelo, J. (2017). Treatment of Severe Hyperkalemia: Confronting 4 Fallacies. Kidney International Reports, 3, 47–55.
https://doi.org/10.1016/j.ekir.2017.10.001
Alaraimi, R., et al. (2020). Variability in practice patterns in the emergency department treatment of hyperkalemia. Canadian Journal of Emergency Medicine, 22.
https://doi.org/10.1017/cem.2020.344
Bonar, P., & Frank, M. (2022). Resolution of Left Bundle Branch Block After Calcium Administration in the Prehospital Setting. Cureus, 14.
https://doi.org/10.7759/cureus.32442
Dépret, F., et al. (2019). Management of hyperkalemia in the acutely ill patient. Annals of Intensive Care, 9.
https://doi.org/10.1186/s13613-019-0509-8
Durfey, N., et al. (2017). Severe Hyperkalemia: Can the ECG Risk Stratify for Short-term Adverse Events? Western Journal of Emergency Medicine, 18, 963–971.
https://doi.org/10.5811/westjem.2017.6.33033
Elmoheen, A., et al. (2020). Severe Persistent Hyperkalemia with Electrocardiogram Changes in a Patient with Hyperaldosteronism. Cureus, 12.
https://doi.org/10.7759/cureus.11358
Geng, S., et al. (2021). Sodium bicarbonate administration and subsequent potassium concentration in hyperkalemia treatment. American Journal of Emergency Medicine, 50, 132–135.
https://doi.org/10.1016/j.ajem.2021.07.032
Gupta, A., et al. (2021). Dispelling myths and misconceptions about the treatment of acute hyperkalemia. American Journal of Emergency Medicine, 52, 85–91.
https://doi.org/10.1016/j.ajem.2021.11.030
Jessen, M., et al. (2025). Pharmacological Interventions for the Acute Treatment of Hyperkalemia: A Systematic Review & Meta-analysis. Resuscitation, 110489.
https://doi.org/10.1016/j.resuscitation.2025.110489
Kreitzer, N., et al. (2025). EMCREG-International Multidisciplinary Consensus Panel on Management of Hyperkalemia. Cardiorenal Medicine, 15, 133–152.
https://doi.org/10.1159/000543385
Lemoine, L., et al. (2021). Evidence-Based Review of ED Management of Acute Hyperkalemia. Journal of Emergency Medicine.
https://doi.org/10.1016/j.jemermed.2020.11.028
Lindner, G., et al. (2020). KDIGO Summary: Acute Hyperkalemia in the Emergency Department. European Journal of Emergency Medicine, 27, 329–337.
https://doi.org/10.1097/mej.0000000000000691
Piktel, J., et al. (2024). Beneficial Effect of Calcium Treatment for Hyperkalemia Is NOT Due to “Membrane Stabilization.” Critical Care Medicine, 52, 1499–1508.
https://doi.org/10.1097/ccm.0000000000006376
Qavi, A., et al. (2020). New Onset Left Bundle Branch Block Secondary to Severe Hyperkalemia. Circulation.
https://doi.org/10.1161/circ.142.suppl_3.15474
Rafique, Z., et al. (2021). Hyperkalemia Management in the ED: Expert Panel Consensus. JACEP Open, 2.
https://doi.org/10.1002/emp2.12572
Sun, J., et al. (2024). Impact of Hyperkalemia on ICU Admission & Mortality: ED Study. BMC Emergency Medicine, 24.
https://doi.org/10.1186/s12873-024-01011-z
Wu, Y., et al. (2023). Treatment & Prognostic Factors in Hyperkalemia in the ED. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue, 35:321–325.
https://doi.org/10.3760/cma.j.cn121430-20220711-00653
Yamanoglu, N., & Yamanoğlu, A. (2022). Effect of Calcium Gluconate in Hyperkalemia. Turkish Journal of Emergency Medicine, 22, 75–82.
https://doi.org/10.4103/2452-2473.342812
Beautiful post. You also covered the lastest article in Critical Care Medicine which proved calcium does not actually stabilise membrane which has been the traditional teaching for decades. One thing to add is: Even in acidotic patients, giving hypertonic bicarbonate doesn't reduce potassium levels. You need to give it as an isotonic solution, otherwise the hypertonicity pulls potassium out of cells, the reverse of which is the mechanism by which bicarbonate works, thereby cancelling each other and potassium levels remain same.
This is so interesting. I didn't know about the ECG correlation to Ca gluconate use. The post is succinct and resourceful. Looking forward to next Hyper K case .