
Acute Care Implications of the 2026 NICE T2DM Update
What EM, CCM and Acute Physicians Must Now Expect

The 2026 revision of NICE NG28 represents a paradigm shift:
glucose-lowering therapy is now anchored to cardio-renal protection, not simply glycaemic control. As a result, the drug profiles of patients presenting to ED/ICU might fundamentally changed.
1. SGLT-2 Inhibitors as Foundational Therapy
What has changed
SGLT-2 inhibitors are now recommended first-line (with metformin) across:
No comorbidity
Heart failure
ASCVD
CKD (down to eGFR 20)
Early-onset T2DM
Obesity
Acute Care Relevance
1.1 Expect near-universal exposure
A large proportion of T2DM patients presenting to ED will be on:
Empagliflozin
Dapagliflozin
This includes patients with:
Advanced CKD (eGFR 20–30, combined with DPP-4 inhibitor)
type-2-diabetes-in-adults-manag…
Heart failure with preserved or reduced EF
ASCVD on triple therapy
1.2 Increased Risk of Eu-glycaemic DKA
The guideline explicitly:
Requires DKA risk assessment before starting SGLT-2
Advises suspension during ketogenic diets and intercurrent illness
EM/ICU Translation
Lower threshold to:
Check blood ketones in:
Sepsis
Major surgery
AKI
Reduced oral intake
Steroid therapy
Diagnose DKA despite glucose <250 mg/dL
Stop SGLT-2 immediately on admission if:
Shock
Hypoxia
AKI
Severe infection
Peri-operative state
Clinical shift: Hyperglycaemia is no longer required to suspect DKA.
2. Sick-Day Rules Become Mandatory Documentation
The updated guideline mandates explicit sick-day plans including temporary cessation of:
Metformin
SGLT-2 inhibitors
Acute Care Implication
In ED/ICU you are now:
Justified in holding these agents in:
Dehydration
Hypotension
Sepsis
Contrast exposure
Expected to document:
When to restart
Under what renal/hemodynamic parameters
Metformin: Stop in hypoxia, shock, significant AKI (lactic acidosis risk).
SGLT-2: Stop early in any catabolic or volume-depleted state.
3. Advanced CKD Patients Will Still Be on SGLT-2
The update allows:
Dapagliflozin or empagliflozin down to eGFR 20
Combination with DPP-4 inhibitor between eGFR 20–30
EM/ICU Implications
You will encounter:
Dialysis-adjacent patients still taking SGLT-2
Lower baseline glucose but ongoing osmotic diuresis risk
Monitor for:
Volume depletion
Hypotension
AKI worsening
Electrolyte shifts
4. Early Triple Therapy is Now Common
For ASCVD, obesity, and early-onset T2DM:
Metformin
SGLT-2 inhibitor
GLP-1 RA or tirzepatide
ICU Implications
Expect:
Lower HbA1c but polypharmacy
Reduced insulin requirements at baseline
Higher GI side-effect burden
5. GLP-1 Receptor Agonists & Tirzepatide in Acute Care
Recommended strongly for ASCVD and obesity
Acute Care Consequences
5.1 Delayed Gastric Emptying
Implications:
Increased aspiration risk
Nausea/vomiting complicating NIV tolerance
Enteral feeding delays
5.2 Peri-intubation considerations
Consider:
Full stomach assumption
RSI preference in unstable patients
6. Glucose Monitoring: Acute Illness and Steroids
The guideline emphasizes:
Acute intercurrent illness increases hyperglycaemia risk
Short-term capillary monitoring is appropriate during steroid initiation
EM/ICU Translation
Expect:
Marked steroid-induced hyperglycaemia
Rapid escalation of insulin requirements
Need for structured monitoring post-discharge
Steroid-treated pneumonia/COPD patients will frequently require:
Basal-bolus insulin
Escalated capillary monitoring
7. Continuous Glucose Monitors (CGM) Use Will Increase in Hospital
Clear endorsement of:
isCGM
rtCGM in insulin-treated T2DM with recurrent/severe hypoglycaemia
Acute Care Implications
You will see:
CGM sensors in admitted patients
Important:
Do NOT rely solely on CGM in:
Shock
Rapid glucose change
Vasopressor states
Capillary testing remains required for accuracy confirmation.
Ensure:
Backup strips are available
Device knowledge confirmed at discharge
8. Organ-Protection Bias Over Glycaemia
The guideline states that SGLT-2 and GLP-1 RAs are recommended as much for CV/renal benefit as glycaemia
Critical Care Reframing
When rationalising medications in ICU:
Do not interpret normal HbA1c as overtreatment.
Instead:
Distinguish glycaemic drugs from organ-protective drugs
Restart SGLT-2 and GLP-1 early once:
Hemodynamically stable
Renal function recovered
Oral intake adequate
These are now secondary prevention agents.
9. Frailty and Hypotension Risk
For frail adults:
SGLT-2 only if low risk of volume depletion/hypotension
ED/ICU Implication
In elderly septic patients:
SGLT-2 may contribute to:
Pre-existing volume contraction
Orthostatic collapse
AKI
High vigilance for polypharmacy-related hypotension.
10. Peri-Operative and Critical Care Protocol Adjustments
Because SGLT-2 use is now foundational:
Every diabetic ICU admission should trigger:
Medication reconciliation focused on SGLT-2
Ketone surveillance if acidosis
Clear peri-operative cessation plan
The era of “metformin only” diabetics is over.
Start/stop decision plan in EM/Acute care
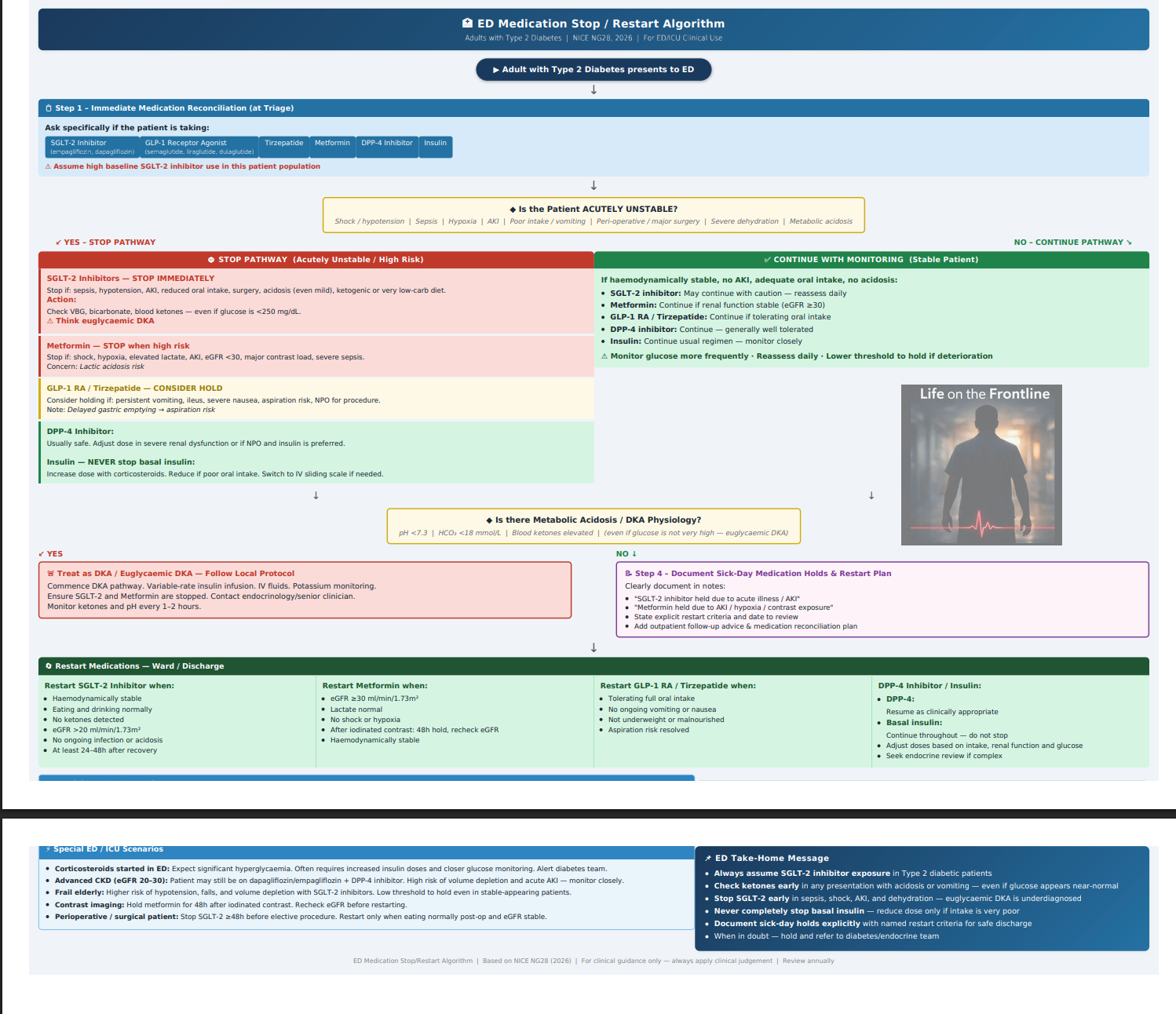
Bedside decision algorithm - for stop/restart of DM drugs in acute care.
For more such updates-
Follow on instagram
References-
NICE 2026 update on T2DM