
ACG 2026 Hepatic Encephalopathy Update
What Emergency & Acute Care Teams Must Change—Starting Tomorrow

Hepatic encephalopathy (HE) is no longer a “late complication.” It is now the most common first decompensating event in cirrhosis—driving ED visits, ICU admissions, readmissions, caregiver burden, and mortality.
The 2026 ACG Clinical Guideline reframes HE as a systems disease, not just a biochemical one. When combined with ACC 2022 ICU care principles, it demands a shift in how we triage, investigate, and treat these patients.
1. HE Is Not “Just Ammonia”
The Three Villages + Five Axes Framework
The guideline introduces a conceptual model that should anchor bedside thinking:
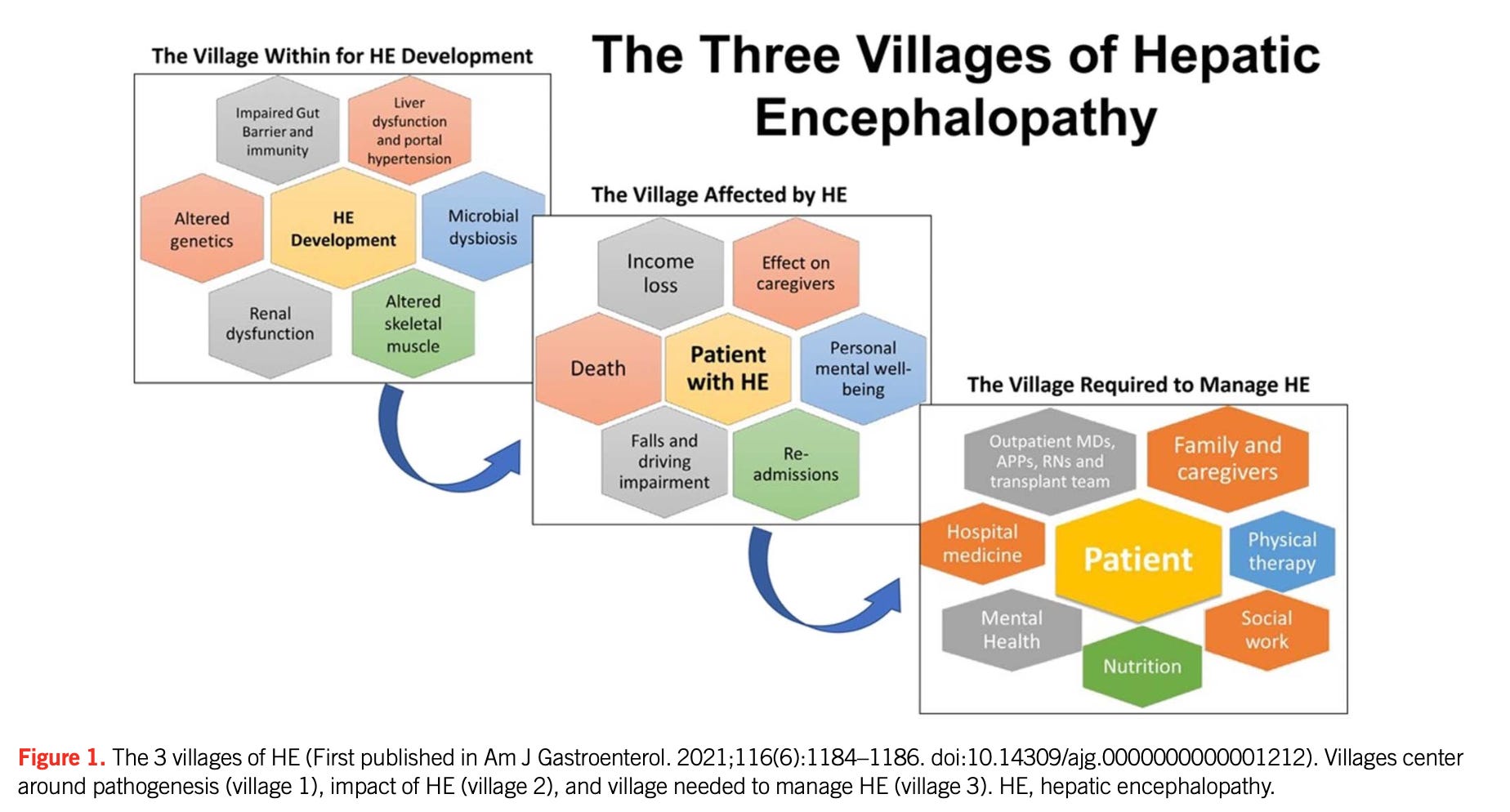
“Three Villages of HE”
Village 1 – Pathogenesis (gut–brain axis, inflammation, ammonia, sarcopenia)
Village 2 – Impact (patients, caregivers, healthcare systems)
Village 3 – Multidisciplinary care (ED, hepatology, ICU, rehab, social systems)
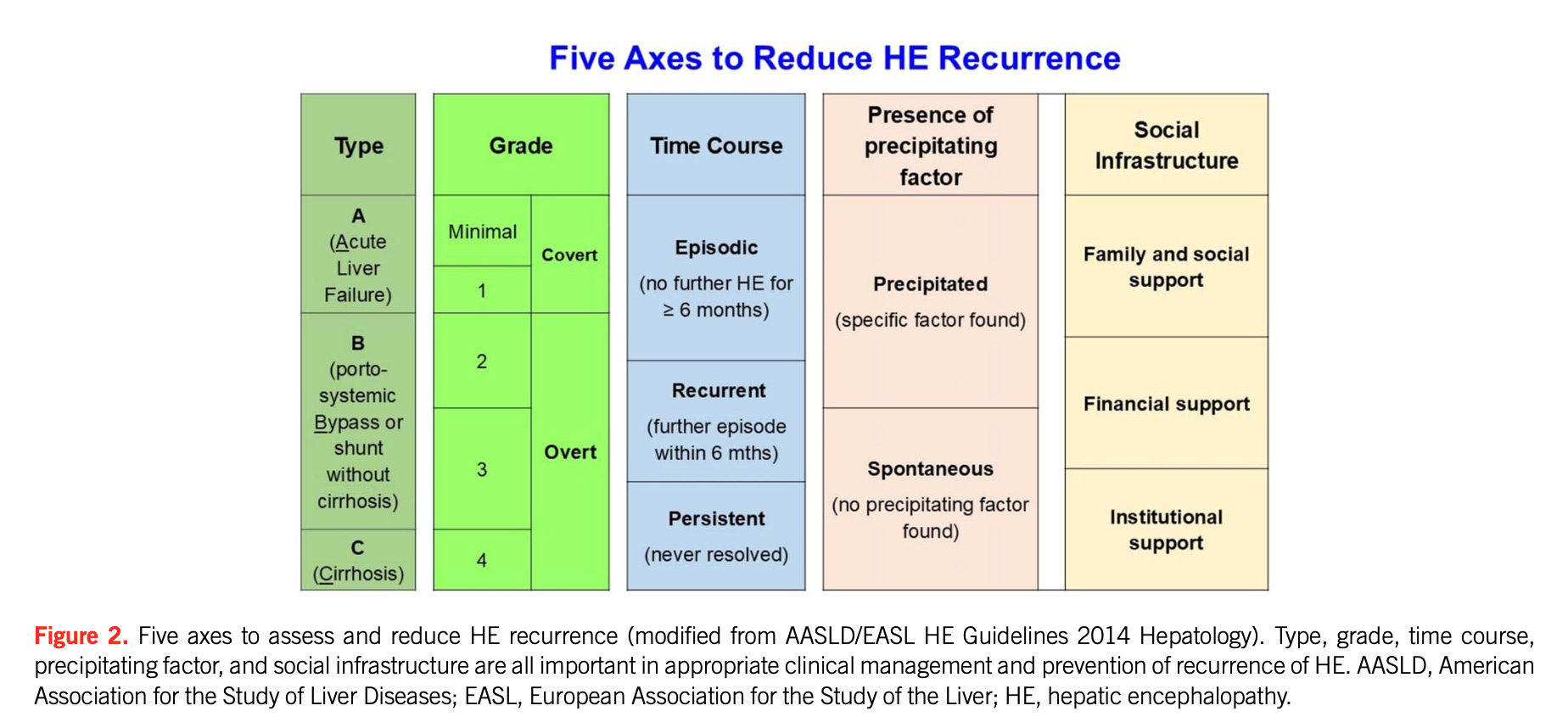
HE is now classified across five axes:
Type (A/B/C)
Severity (West Haven)
Time course
Precipitated vs non-precipitated
Social infrastructure (NEW)
👉 Game changer:
You must now ask:
“Can this patient actually survive outside the hospital?”
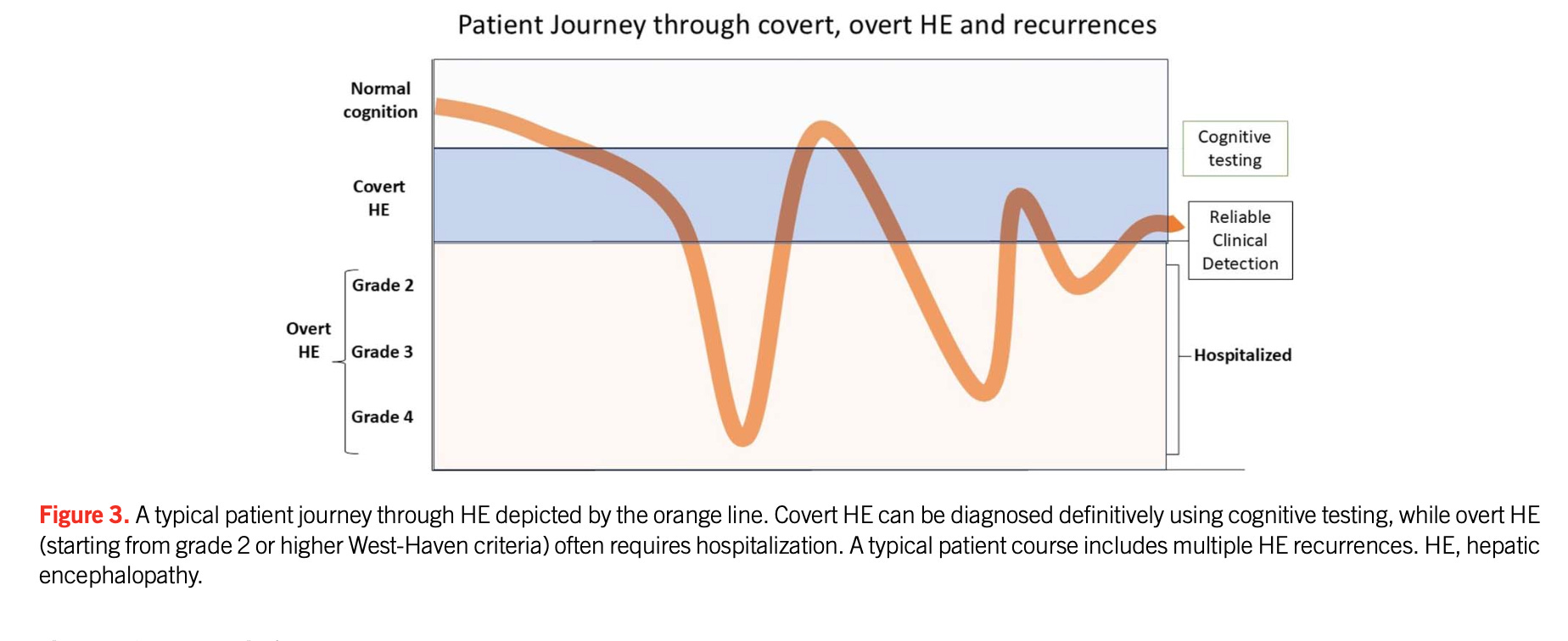
Covert HE → Overt HE → Recurrent admissions → Cognitive decline
ED clinicians often see patients too late in this curve
2. Covert/Minimal HE (CHE/MHE): The Missed Diagnosis in ED
Who should trigger suspicion?
Hypoalbuminemia
Decompensated cirrhosis
Portal hypertension/shunts
Falls, traffic violations, navigation issues
Subtle cognitive complaints
👉 Key ED pearl:
Isolated asterixis ≠ OHE
How to test (NOT ammonia)
Single-test strategy (ACG recommendation)
Practical tools:
Stroop / EncephalApp
Animal Naming Test
Critical Flicker Frequency
❌ Do NOT use ammonia to diagnose CHE
Treatment: “Theragnostic trial”
Lactulose (4–8 week trial)
Reassess cognition + function
Useful in ED follow-up planning and liaison clinics
3. “Is This Really HE?” — The Cognitive Differential
“Cirrhosis + Cognitive Complaint Pathway”
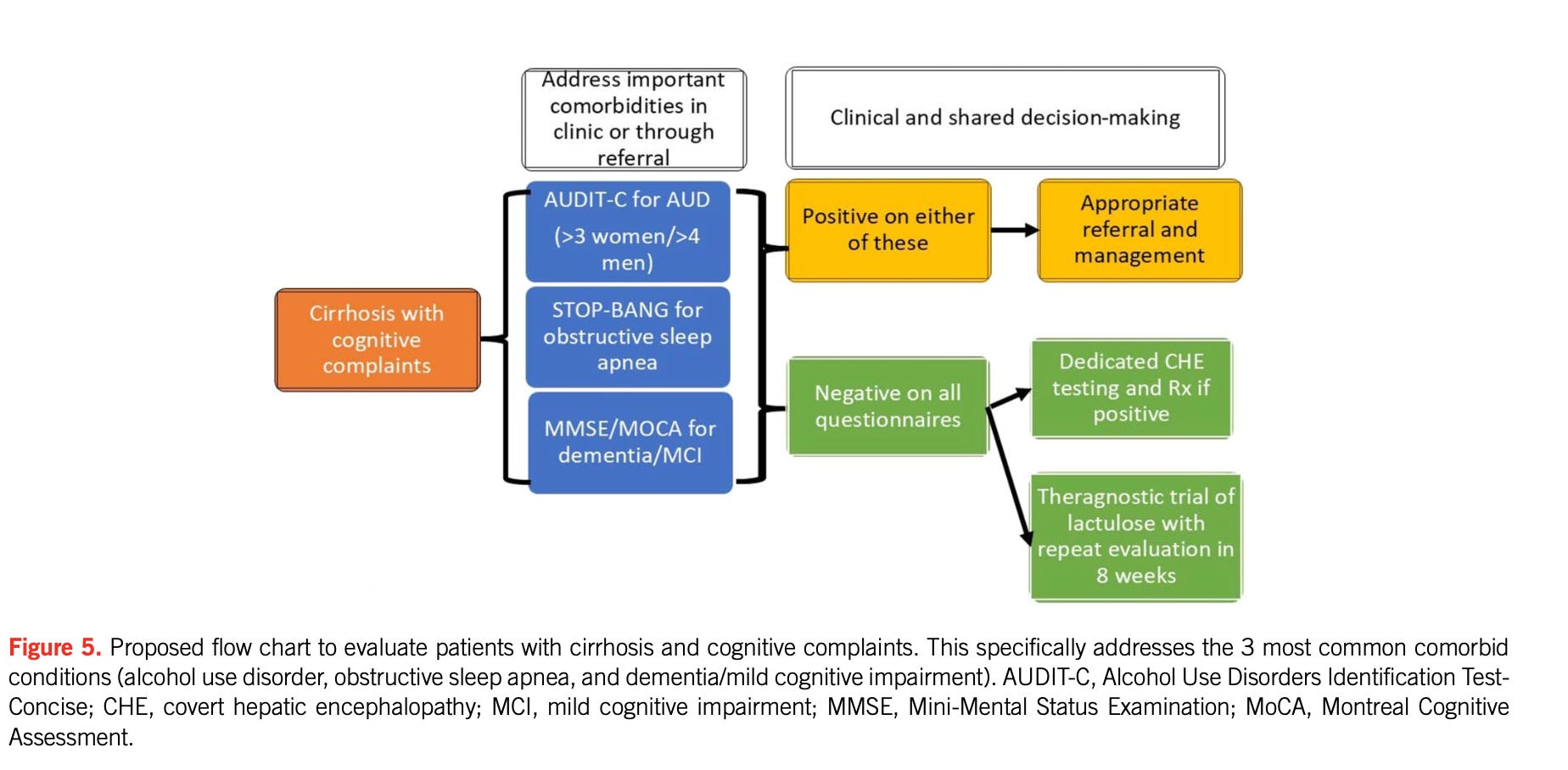
More than 50% of suspected HE ≠ HE
Common mimics:
Dementia / MCI
Depression / PTSD
Obstructive sleep apnea
Substance use
Metabolic/endocrine disorders
👉 ED shift:
Stop reflex lactulose escalation → start structured differential evaluation
4. Overt HE in ED & ICU
Triage: Who Needs Admission?
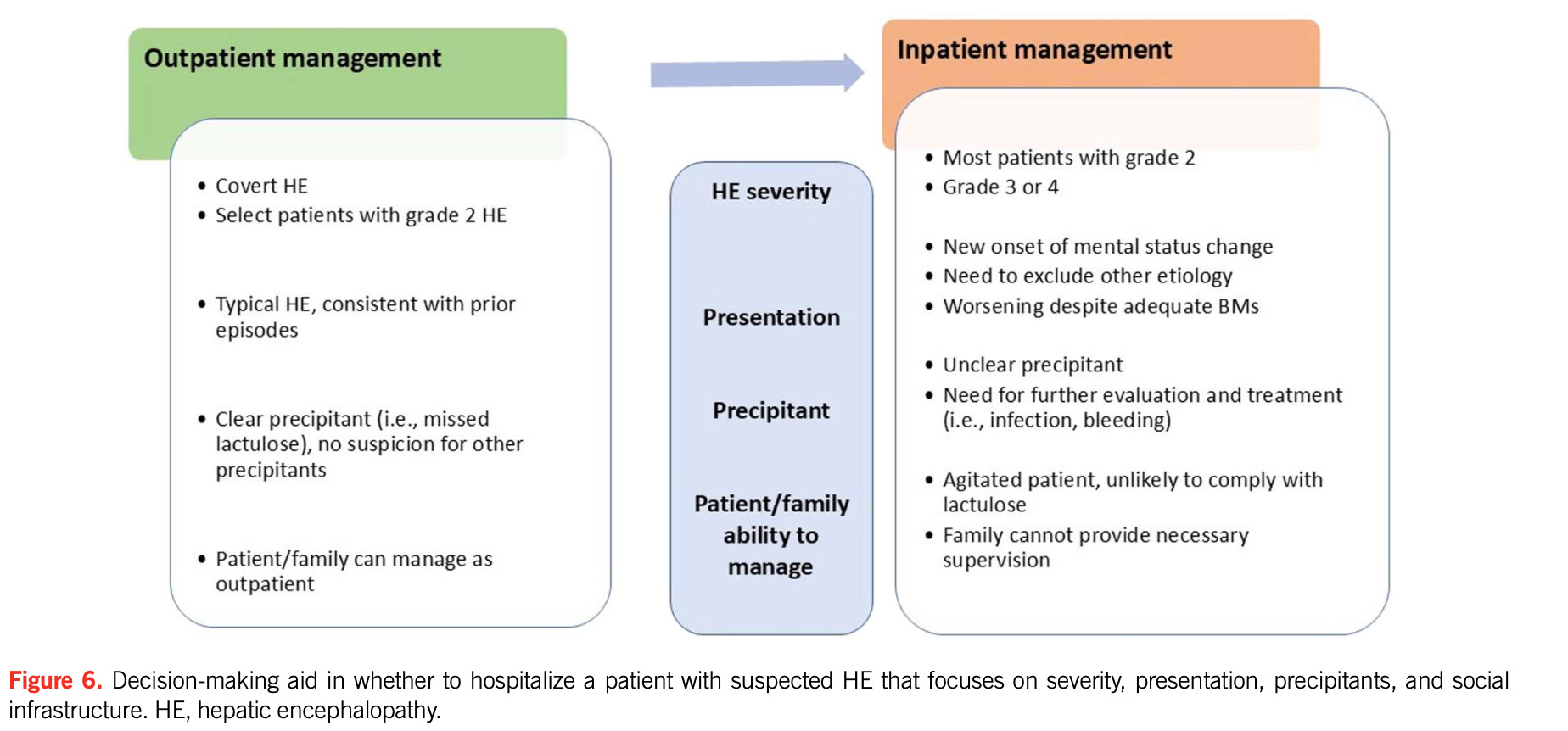
“Admission Decision Flowchart”
Admit if:
Grade 3–4 HE
First episode
Infection, bleed, AKI
Poor social support
Strong Recommendations That Change Practice
Lactulose for OHE (strong)
Secondary prophylaxis after first episode (strong)
Add rifaximin for recurrence (strong)
Protein 1.2–1.5 g/kg/day (strong)
Branched Chain Amino Acid (BCAA) —> if needed (strong)
Rifaximin pre-TIPS (strong)
🚨 What to STOP Doing
Routine ammonia testing
Routine CT brain without focal deficit
👉 A normal ammonia ≠ no HE
👉 HE = clinical diagnosis of exclusion
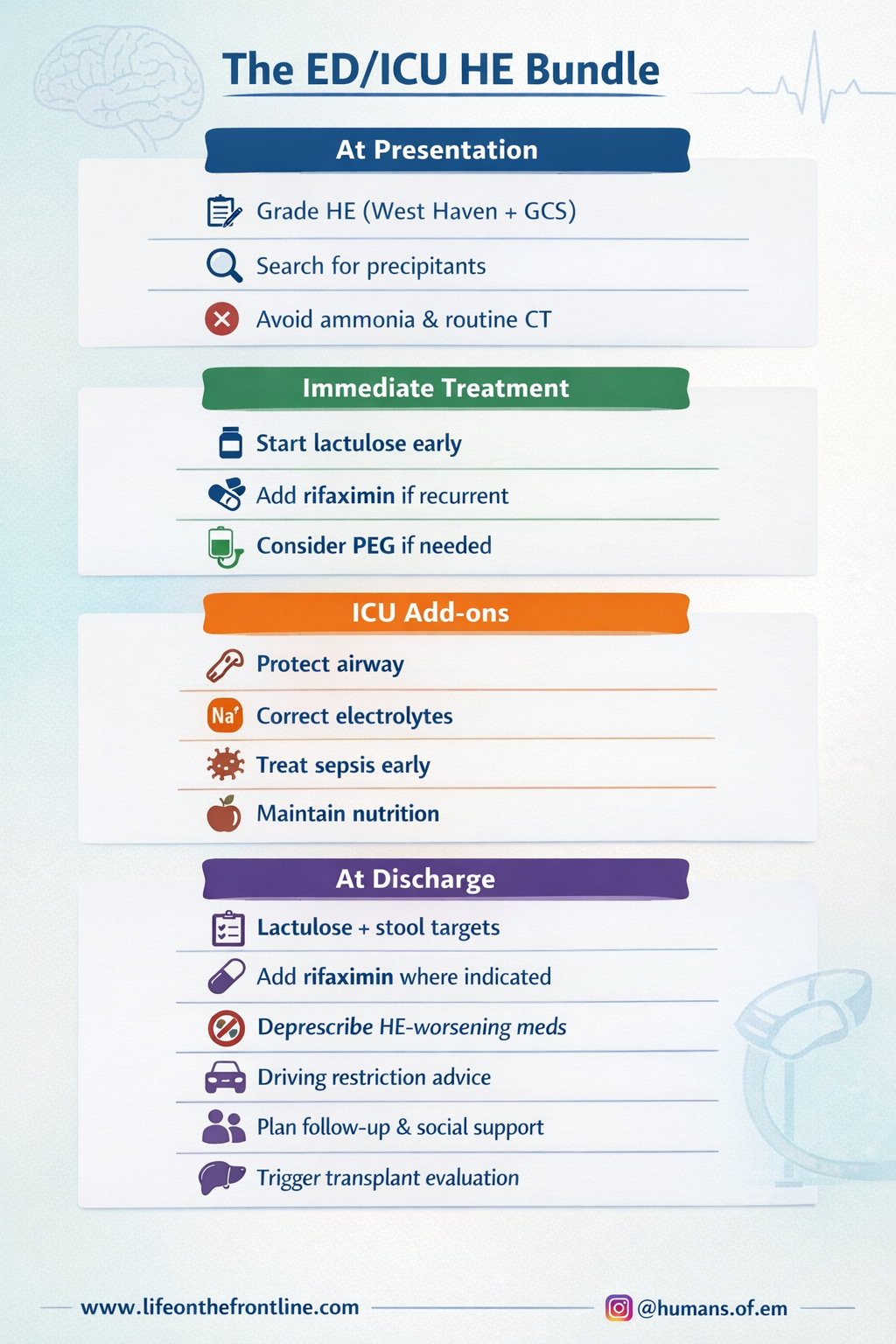
5. Acute Management: ED + ICU Integration (ACG 2026 + ACC 2022)
Acute HE Treatment Algorithm
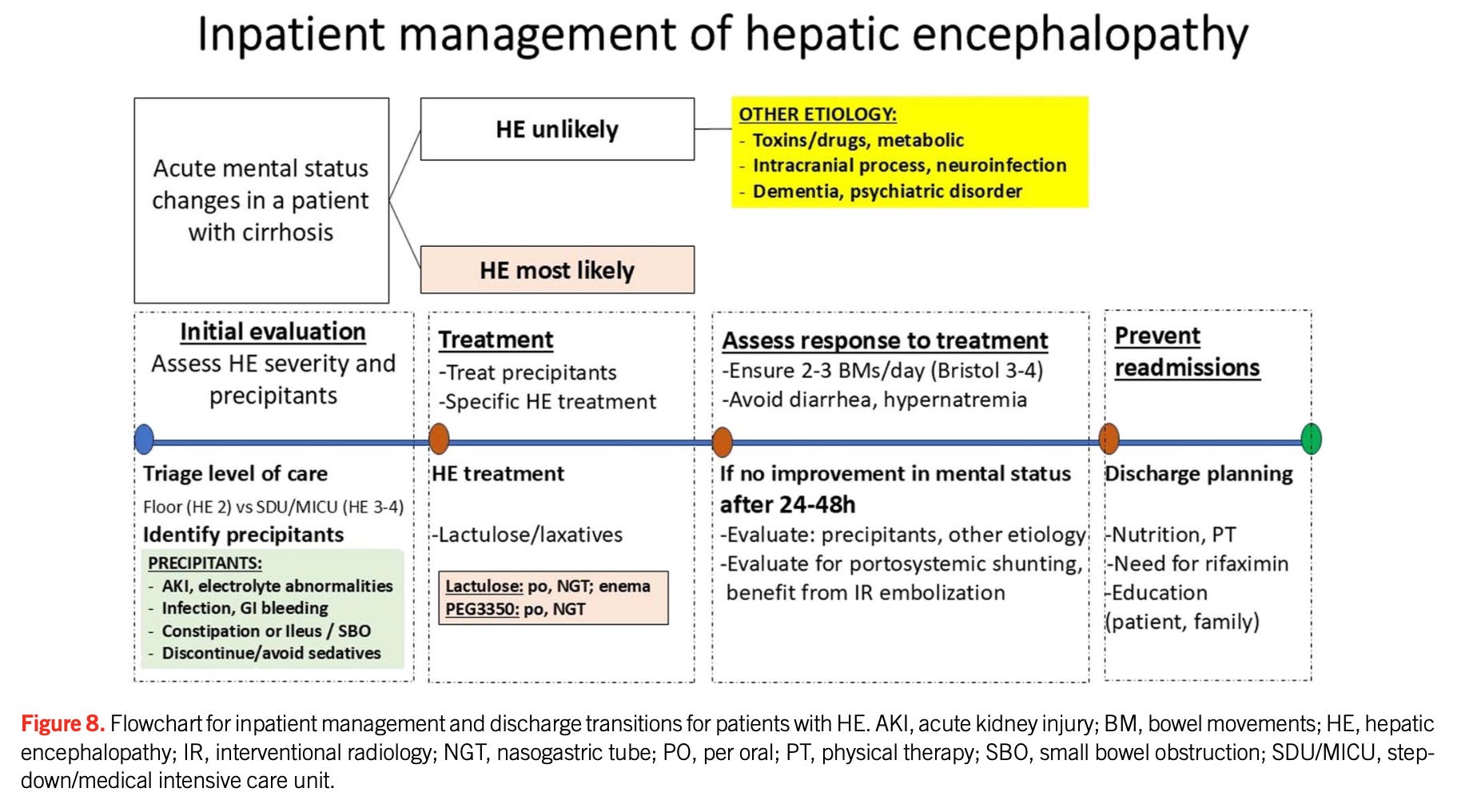
First-line (ED + ICU)
Lactulose
Oral/NG: every 1–2 hrs → 2–3 soft stools
Enema if needed
⚠️ Avoid overuse → dehydration, hypernatremia
See more about Lactulose in HE, here
PEG (Alternative)
Faster resolution in trials
Useful if ileus/bloating
Rifaximin
Add in recurrent HE
Consider early in severe ICU cases
ACC 2022 ICU Principles (Add These to Your Workflow)
Airway & Neuroprotection
Intubate if:
GCS ≤ 8
Aspiration risk
Avoid oversedation (benzodiazepines worsen HE)
Hemodynamic & Metabolic Targets
Maintain MAP ≥ 65 mmHg
Correct:
Hypokalemia
Hyponatremia
Hypoglycemia
Infection Control
Low threshold for antibiotics
Sepsis = major precipitant
ICP & Cerebral Edema (Severe HE / ACLF)
Head elevation
Avoid hypercapnia
Consider hypertonic saline if needed
Nutrition (Critical Update)
DO NOT restrict protein
ICU patients may need up to 2 g/kg/day
6. Nonresponse at 48–72 Hours
📌 Insert Figure 9 here – “Nonresponse Algorithm”
If not improving:
Reconsider diagnosis
Re-look for precipitants
Evaluate for:
TIPS
Large shunts
👉 Do NOT just increase lactulose blindly
7. Preventing Recurrence
“Recurrence Prevention Pathway”
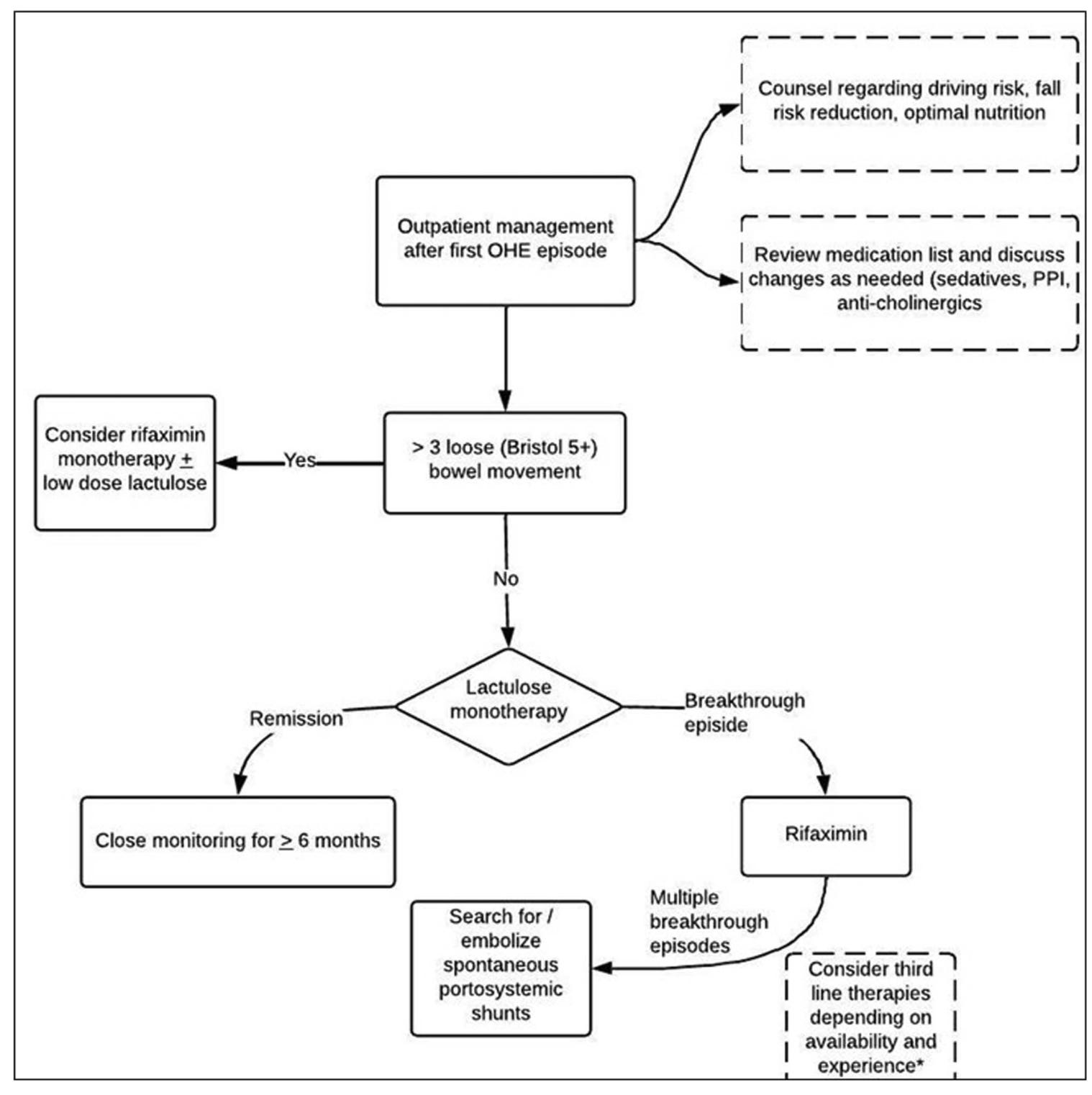
Core Strategy
Lactulose (target 2–3 stools/day)
Rifaximin (↓ recurrence 58%)
System-Level Changes
Use Bristol stool scale
EMR alerts/order sets
Patient education tools
Deprescribing (Critical ED Role)
Stop/minimize:
Benzodiazepines
Opiates
Gabapentinoids
Z-drugs
PPIs (when inappropriate)
Nutrition & Sarcopenia
Protein: 1.2–1.5 g/kg/day
Late-night snack
Exercise programs
👉 Muscle = ammonia buffer
8. TIPS, Refractory HE & Transplant
TIPS-related HE
Start rifaximin 14 days before TIPS
Continue ≥ 6 months
Refractory HE
Consider:
Shunt embolization
TIPS revision
Transplant Implications
HE underestimates MELD risk
Consider transplant even at low MELD
👉 Early referral if:
Recurrent HE
Grade III–IV
Persistent cognitive decline
Follow us on Instagram: @humans.of.em
References
Bajaj JS, Jakab SS, Jesudian AB, et al. ACG Clinical Guideline: Hepatic Encephalopathy. Am J Gastroenterol. 2026;121:588-618. doi:10.14309/ajg.0000000000003899
Vilstrup H, Amodio P, Bajaj J, et al. Hepatic Encephalopathy in Chronic Liver Disease: 2022 Practice Guidance. Hepatology. 2022;76(3):1027-1040. doi:10.1002/hep.32477
great post thank you. Does that mean we should not start Rifaximin for all cases of HE that is grade 2 or higher
👍