
A Bayesian Lens on a Reversible “High-Risk” ECG
Interpreting ACS–Like ECG Patterns Through Pre-Test Probability

If you saw this ECG ,
aVR ST elevation.
V1 ST Segment elevated in comparison to V2.
Diffuse ST depression.
New right axis deviation.
your first instinct would probably be left main or proximal LAD occlusion.
Ours too.
But this case turned out to be a powerful reminder that ECG interpretation in Emergency Medicine is Bayesian — not binary.
The meaning of any ECG depends on the pre-test probability, the clinical context, and the physiology beneath it.
And in this patient, the entire picture shifted when we learned one critical detail:
He had an acute upper GI bleed earlier that day — approximately 1 liter.
ECG 1 was taken shortly after this massive blood loss.
And after correcting the reversible physiologic insult, the ECG normalized completely.
This post walks through the reasoning, the differentials, and what this ECG really means in an ED setting.
ECG 1: The Concerning Findings
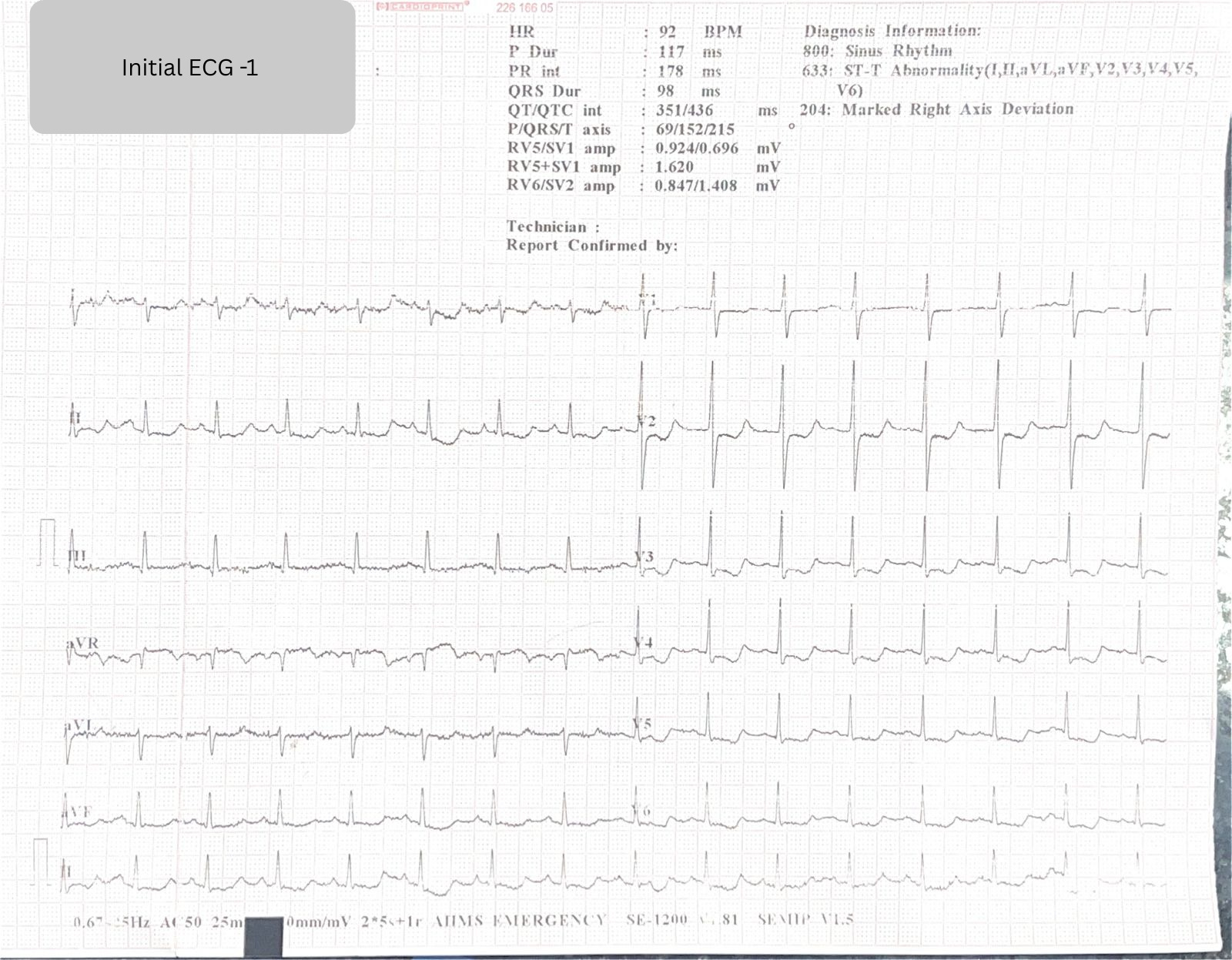
The initial ECG showed:
aVR ST elevation
V1 > V2 ST segment level
Diffuse ST depression
New right axis deviation (Lead I isoelectric/negative vs. ECG 2)
This pattern is alarming because it mimics:
Proximal LAD occlusion
Left main disease
Severe multivessel ischemia
But ECGs don’t diagnose ACS — they shift probability.
The patient’s physiology completes the story.
The Clinical Context:
This patient had a fresh bout of ~1 L blood loss from an upper GI bleed a few hours before arriving in the ED.
Acute hemorrhage →
↓ oxygen delivery
↓ preload
↓ coronary perfusion pressure
↑ myocardial oxygen demand
↑ sympathetic surge
This is the perfect storm for global subendocardial ischemia — a condition that mimics ACS on ECG but is fully reversible.
And in this case, it was.
ECG 2
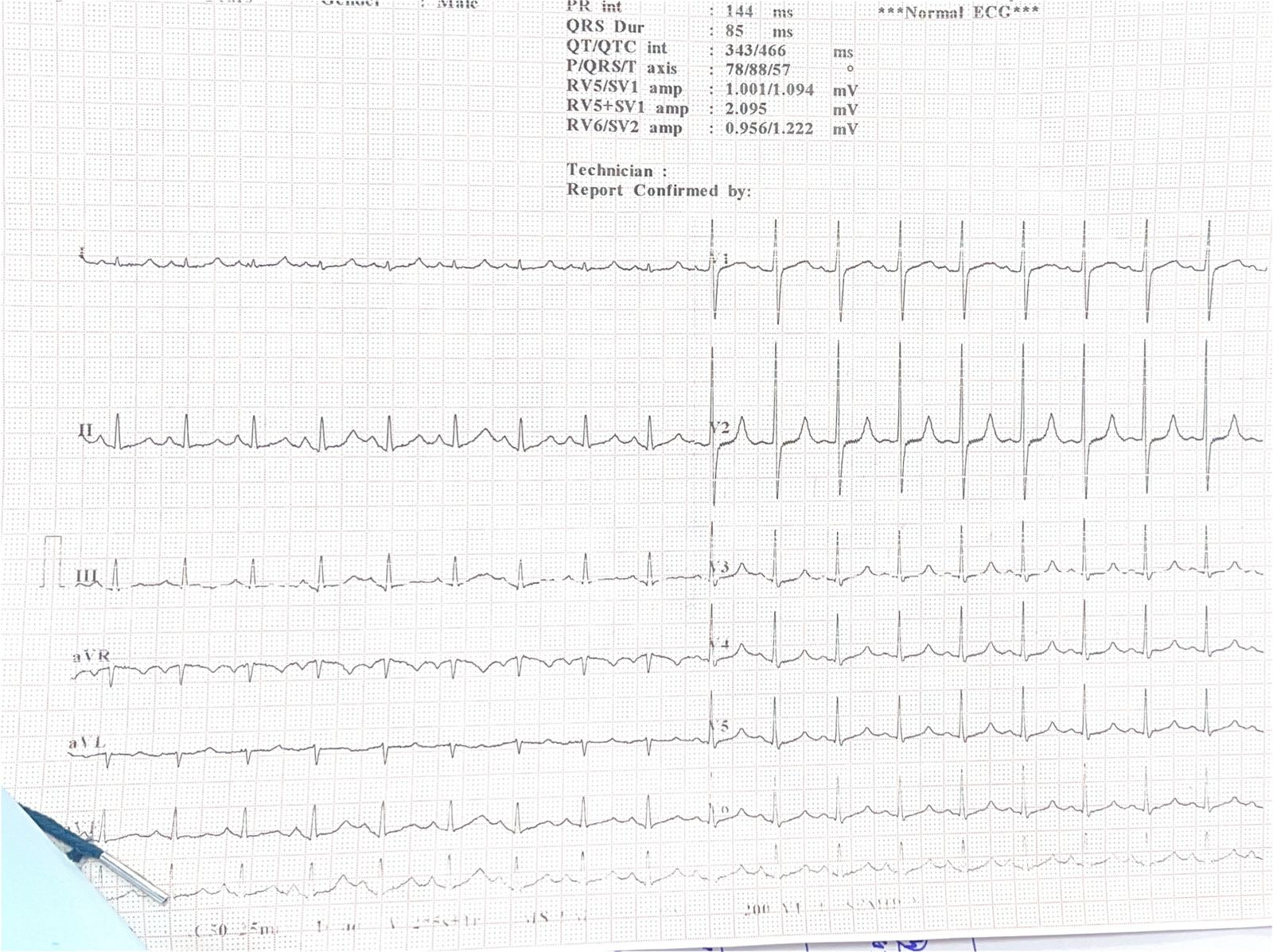
After stabilizing the patient and correcting the physiologic derangement:
ST depressions resolved
aVR ST elevation normalized
V1/V2 changes disappeared
Axis returned to baseline
Understanding These ECG Patterns Through a Bayesian Lens
When encountering this pattern:
aVR ST elevation
Diffuse ST depression
V1 > V2 ST elevation
Axis shift
you must evaluate the pre-test probability of ACS
These ECG features have:
High sensitivity for global ischemia
Low specificity for ACS
Moderate LR+ only when the patient already has a high ACS likelihood
So your clinical judgment determines how much the ECG moves your post-test probability.
A Practical ED Framework: How to Approach This ECG
1. If Pre-Test Probability of ACS Is HIGH
Treat as ACS until proven otherwise.
This includes patients with:
Classic ischemic symptoms
High-risk CAD profile
Hemodynamic instability
Concerning echo findings
High clinical suspicion
This ECG may represent:
Precordial swirl pattern
Proximal LAD occlusion
Left main equivalent
Immediate steps:
POCUS for RWMA
Repeat ECGs
ACS pathway activation
Stabilization + consults
(References: Harhash 2019; Bhatt 2022; Ricci 2025)
2. If Pre-Test Probability of ACS Is LOW
Rule out other causes first — especially reversible, physiologic ones.
Use:
POCUS (heart, lungs, IVC)
ABG/VBG (pH, lactate, bicarbonate)
Electrolytes
Hb level
Focused history (bleeding, toxins, hypoxia, PE risk)
If no reversible cause emerges →
reconsider ACS and escalate accordingly.
(References: Bouzid 2022; Choi 2022; Y-Hassan 2020)
Differential Diagnosis: Why This ECG Is Not Always ACS
This pattern often reflects sub-endocardial ischemia or metabolic stress.
1️⃣ Perfusion Supply–Demand (S/D) mismatch
Severe anemia
Shock
Hypoxia
Tachycardia (can unmask CAD)
Acute blood loss ← the cause in this case
(References: Bouzid 2022; Al-Zaiti 2020; Y-Hassan 2020)
2️⃣ Pulmonary Embolism
RAD
V1 > V2 elevation
RV strain patterns
(References: Harhash 2019; Y-Hassan 2020)
3️⃣ Severe Aortic Stenosis
4️⃣ Aortic Dissection
5️⃣ Metabolic Causes
Hypokalemia
Severe metabolic acidosis
Sodium channel blocker toxicity
All can mimic ischemia — and all can resolve with treatment.
(References: Y-Hassan 2020; Hong & Zeng 2022)
Serial ECGs + POCUS = Diagnostic Power Tools
Literature consistently supports:
Serial ECGs identify transient or reversible changes (Bouzid 2022; Choi 2022)
POCUS rapidly shifts probability up or down
Dynamic improvement → strong evidence against ACS
Persistent abnormalities → significantly raises ACS probability
This is bedside Bayesian reasoning in action.
Final Takeaway
An ischemic-looking ECG does not always mean ACS.
With the right clinical context — like acute hemorrhage — these changes may be entirely reversible.
What matters most is:
The pre-test probability
The physiology
Bedside imaging
Response to treatment
Serial ECG trends
In Emergency Medicine, pattern recognition is essential.
But pattern + probability is what saves lives.
References:
Bouzid Z, Faramand Z, Martin-Gill C, Sereika S, Callaway C, Saba S, et al. Incorporation of serial 12-lead electrocardiogram with machine learning to augment the out-of-hospital diagnosis of non-ST elevation acute coronary syndrome. Ann Emerg Med. 2022. doi:10.1016/j.annemergmed.2022.08.005
Choi Y, Lee J. Dynamic changes in electrocardiographic findings between initial and follow-up electrocardiography: The role of the T/QRS ratio. Am J Emerg Med. 2022;54:8-14. doi:10.1016/j.ajem.2022.01.033
Bhatt D, Lopes R, Harrington R. Diagnosis and treatment of acute coronary syndromes: A review. JAMA. 2022;327(7):662-75. doi:10.1001/jama.2022.0358
Harhash A, Huang J, Reddy S, Natarajan B, Balakrishnan M, Shetty R, et al. aVR ST segment elevation: Acute STEMI or not? Incidence of an acute coronary occlusion. Am J Med. 2019;132(5):622-30. doi:10.1016/j.amjmed.2018.12.021
Ricci F, Martini C, Scordo D, Rossi D, Gallina S, Fedorowski A, et al. ECG patterns of occlusion myocardial infarction: A narrative review. Ann Emerg Med. 2025. doi:10.1016/j.annemergmed.2024.11.019
Al-Zaiti S, Besomi L, Bouzid Z, Faramand Z, Frisch S, Martin-Gill C, et al. Machine learning-based prediction of acute coronary syndrome using only the pre-hospital 12-lead electrocardiogram. Nat Commun. 2020;11:3966. doi:10.1038/s41467-020-17804-2
Hong J, Zeng Z. Predictive value of ST-segment deviation in aVR in patients suffering from acute coronary syndrome: A retrospective cohort study. Medicine (Baltimore). 2022;101(5):e29994. doi:10.1097/MD.0000000000029994
Y-Hassan S, Falhammar H. Cardiovascular manifestations and complications of pheochromocytomas and paragangliomas. J Clin Med. 2020;9(8):2435. doi:10.3390/jcm9082435